🧠 Internuclear Ophthalmoplegia (INO) is a brainstem disorder characterised by impaired horizontal eye movement due to a lesion in the medial longitudinal fasciculus (MLF).
👁️ The key finding: failure of adduction of one eye with nystagmus of the abducting eye when looking laterally.
📖 About
- The medial longitudinal fasciculus (MLF) is a paired white matter tract that coordinates horizontal gaze by linking the abducens nucleus (cranial nerve VI) in the pons to the oculomotor nucleus (cranial nerve III) in the midbrain.
- This interconnection ensures synchronous movement of both eyes - essential for binocular vision and depth perception.
- Disruption of the MLF causes failure of one eye to adduct while the other abducts normally with nystagmus.
🧩 Aetiology & Pathophysiology
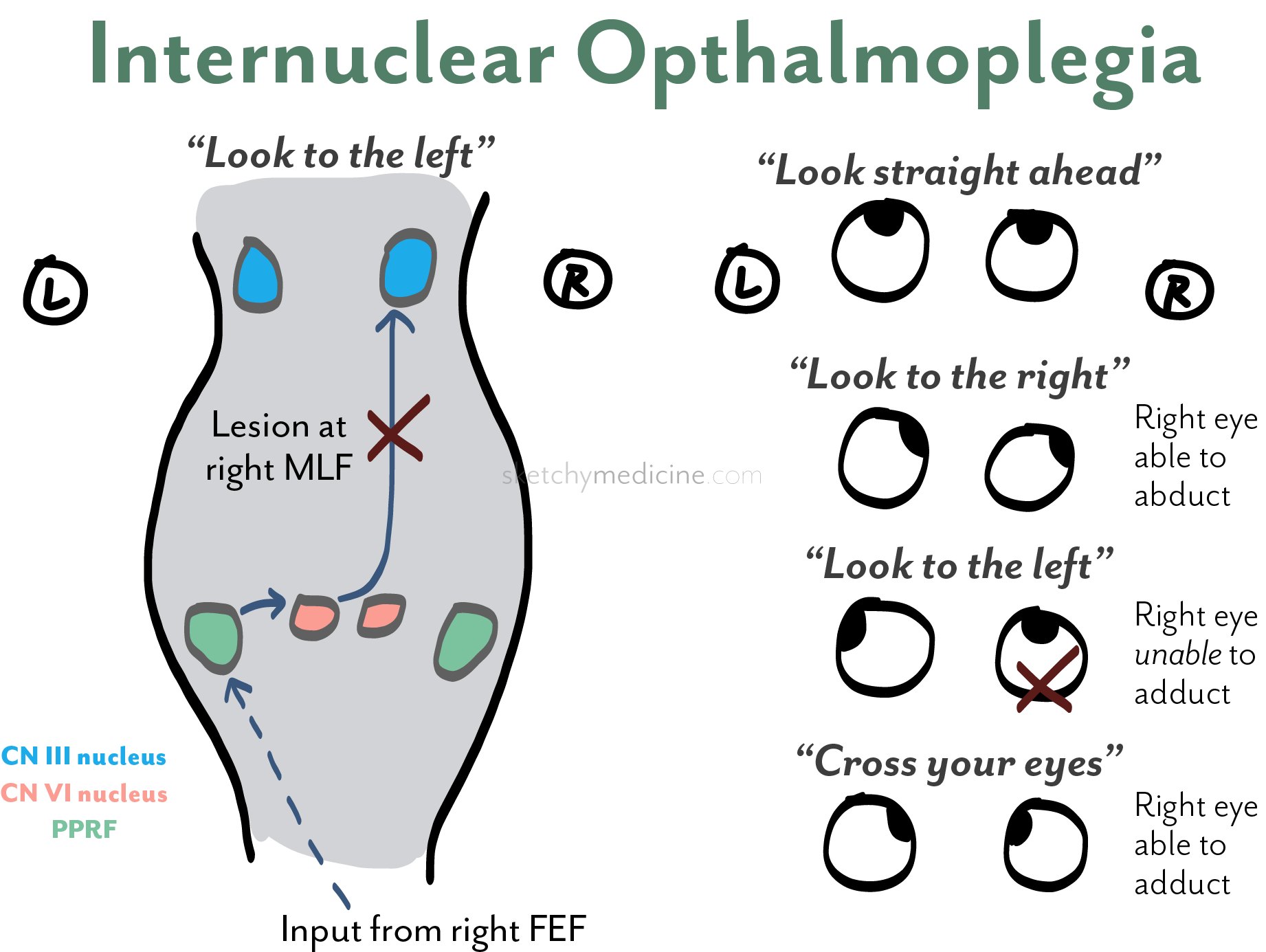
- Normal coordination: When looking left, the left abducens nucleus activates the left lateral rectus and simultaneously sends a signal via the right MLF to the right oculomotor nucleus (to contract the right medial rectus).
- Lesion: Damage to the right MLF prevents transmission of this signal → right eye fails to adduct on left gaze.
- Because the abducting eye receives unopposed input, it overshoots and develops nystagmus.
- In bilateral lesions (often in MS), both MLF tracts are affected, producing bilateral INO - patients often complain of oscillopsia (visual “shaking”).
🧠 Diagram
🩺 Causes
- Multiple Sclerosis (MS): The most common cause in younger adults. Demyelination interrupts conduction within the MLF.
- Brainstem Stroke: Common cause in older adults; usually unilateral and due to infarction of pontine perforators.
- Brainstem Tumours: E.g. glioma, metastasis - compress or infiltrate the MLF.
- Trauma: Brainstem contusion or diffuse axonal injury.
- Inflammatory/Infective: Encephalitis, sarcoidosis, or lupus cerebritis.
🧭 Clinical Features
- Primary gaze: Eyes usually aligned.
- On attempted lateral gaze:
- Abducting eye moves fully but shows nystagmus.
- Adducting eye fails or lags (impaired medial rectus function).
- Lesion localisation: Defective adduction in the left eye = left MLF lesion.
- Bilateral INO: Typically due to MS - both eyes show impaired adduction and bilateral nystagmus.
- “One-and-a-half syndrome”: INO + conjugate gaze palsy to one side due to larger pontine lesion involving both the MLF and ipsilateral PPRF (paramedian pontine reticular formation).
- Convergence: Usually preserved (the medial rectus pathway for convergence bypasses the MLF).
⚖️ Differentials
- Myasthenia Gravis: Can mimic INO (“pseudo-INO”) due to fatigable medial rectus weakness - distinguish by normal convergence and variable findings.
- Third Nerve Palsy: Produces adduction failure but also ptosis and pupil involvement.
- Pontine Lesion: May produce associated contralateral hemiparesis or facial weakness.
🔍 Investigations
- MRI Brainstem: Preferred imaging modality to detect demyelination, infarct, or mass lesion affecting the MLF.
- Consider CSF analysis if demyelination or infection suspected (e.g. oligoclonal bands in MS).
- Autoimmune and vasculitic screen if cause unclear.
🩹 Management
- Treat the underlying cause:
- MS: Corticosteroids for relapse; disease-modifying therapy long term.
- Stroke: Antiplatelet or anticoagulant therapy as indicated.
- Infection/inflammation: Appropriate antimicrobial or immunosuppressive therapy.
- Diplopia can be managed with prism glasses or occlusion therapy in selected patients.
- Physiotherapy and neuro-ophthalmology review for persistent visual dysfunction.
📖 Educational Summary
Internuclear ophthalmoplegia is a classic localising sign of brainstem pathology.
The MLF acts as the “communication cable” between cranial nerves VI and III - when cut, the eyes lose synchrony.
A simple rule for students: the eye that won’t adduct is on the same side as the lesion.
INO also exemplifies how demyelination impairs conduction rather than destroying neurons - explaining why recovery may be good in MS but limited after stroke.
Always differentiate from myasthenia and third nerve palsy, and link the lesion to its neuroanatomical substrate.
📚 References
- BNF: Neurology & MS Management
- BMJ Best Practice: Internuclear Ophthalmoplegia (2023)
- Clinical Neuroanatomy, Snell (9th ed.) – Brainstem Pathways
- Adams & Victor’s Principles of Neurology, 12th ed.
