
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Brain MRI Collection
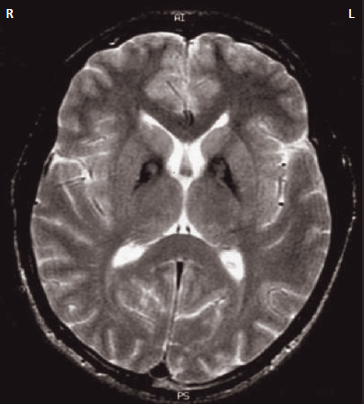
Eye of the Tiger Sign
🐯🧠 What it means: Classic MRI pattern seen in PKAN (Pantothenate Kinase–Associated Neurodegeneration), part of the NBIA disorders.
🧲 Expected imaging findings:
• On T2-weighted MRI: central hyperintensity in the globus pallidus surrounded by hypointensity from iron deposition (“eye of the tiger”).
• The peripheral low signal reflects iron accumulation; the central bright area reflects gliosis/vacuolisation.
🩺 Clinical context: childhood/teen onset dystonia, parkinsonism, spasticity, dysarthria ± cognitive/psychiatric features.
⚠️ Pearl: Similar patterns can rarely be seen in other NBIA conditions, but this sign is strongly associated with PKAN.
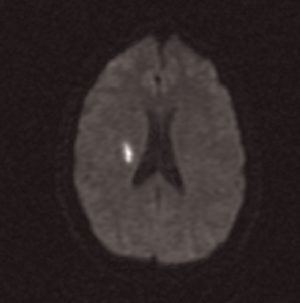
Lacunar Stroke
🧠 Expected imaging findings:
• Small (<15 mm) deep infarcts due to small vessel lipohyalinosis.
• Common sites: internal capsule, basal ganglia, thalamus, pons.
• CT may be normal early; later shows small hypodense cavity (“lacune”).
• MRI DWI is most sensitive acutely (restricted diffusion).
🎯 Classic syndromes: pure motor, pure sensory, ataxic hemiparesis, dysarthria-clumsy hand.
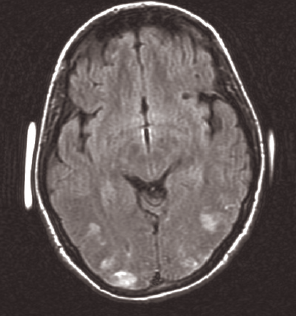
PRES (Posterior Reversible Encephalopathy Syndrome)
⚡ Expected imaging findings:
• Symmetric vasogenic oedema in posterior regions (parieto-occipital lobes) on MRI FLAIR/T2.
• Often subcortical predominance; can involve frontal lobes, cerebellum, brainstem.
• Typically no restricted diffusion (helps distinguish from infarct), though severe cases may show mixed patterns.
• Causes: severe hypertension, eclampsia, renal failure, sepsis, cytotoxic/immunosuppressive drugs.
🚨 Presents with headache, seizures, visual disturbance, encephalopathy - treat trigger and BP.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery