
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Hypothyroidism ✅
Related Subjects: |Thyroid Cancer |Thyroid Eye Disease |Thyroid Function Tests and antibodies |Thyroid Storm - Thyrotoxic crisis |Thyroid Surgery (Thyroidectomy) |Thyroid nodules |Thyrotoxicosis and Hyperthyroidism |Hypothyroidism
💡 Always start with a lower dose of levothyroxine in the elderly or in patients with angina/heart failure to avoid arrhythmia or myocardial ischaemia.
📖 Introduction
- The thyroid secretes mainly T4; most T3 is produced by peripheral conversion.
- Primary hypothyroidism: thyroid failure → TSH ↑, FT4 ↓.
- Secondary/central hypothyroidism: pituitary/hypothalamic disease → TSH low/normal, FT4 ↓; monitor using FT4 and symptoms.
⚙️ Aetiology
- Primary hypothyroidism: autoimmune (Hashimoto's), post-thyroidectomy/radioiodine/radiotherapy, drugs (lithium, amiodarone), thyroiditis, infiltrative, congenital.
- Secondary/central: pituitary/hypothalamic tumours, surgery, radiotherapy, apoplexy, infiltrative disease.
🧑⚕️ Clinical Features
- General: fatigue, lethargy, weight gain, cold intolerance ❄️
- Neuropsychiatric: poor concentration, low mood, psychomotor slowing 🧠
- GI: constipation 🍽️
- Reproductive: menorrhagia, subfertility 👩🦰
- Skin/hair: dry skin, brittle hair, hair loss, hoarse voice, periorbital puffiness 💇♀️
- Cardio: bradycardia, risk of heart failure, pericardial effusion ❤️
- Neuro exam: slow-relaxing reflexes (“hung-up”), proximal myopathy 💪
- Severe: myxoedema coma ❄️🛌 (rare, emergency)
🆚 Differential Diagnosis
- Depression, chronic fatigue, sleep apnoea 😴
- Anaemia, chronic kidney disease, chronic inflammatory disease
- Central hypothyroidism if FT4 low but TSH not elevated
🔬 Investigations (NICE / UK approach)
- First-line: TSH (and FT4 if TSH abnormal or central hypothyroidism suspected)
- Overt primary: TSH ↑, FT4 ↓
- Subclinical: TSH ↑, FT4 normal → repeat in ~3 months
- Thyroid antibodies: TPO Ab supports autoimmune cause
- Other tests: FBC, lipids, B12/folate if indicated
- Imaging: thyroid ultrasound only if structural concerns
📊 Classification
- Overt primary: TSH ↑, FT4 ↓ → treat with levothyroxine 💊
- Subclinical: TSH ↑, FT4 normal → confirm persistence; treat if TSH ≥10 or symptomatic
- Secondary/central: FT4 ↓, TSH low/normal → monitor and treat guided by FT4 & symptoms
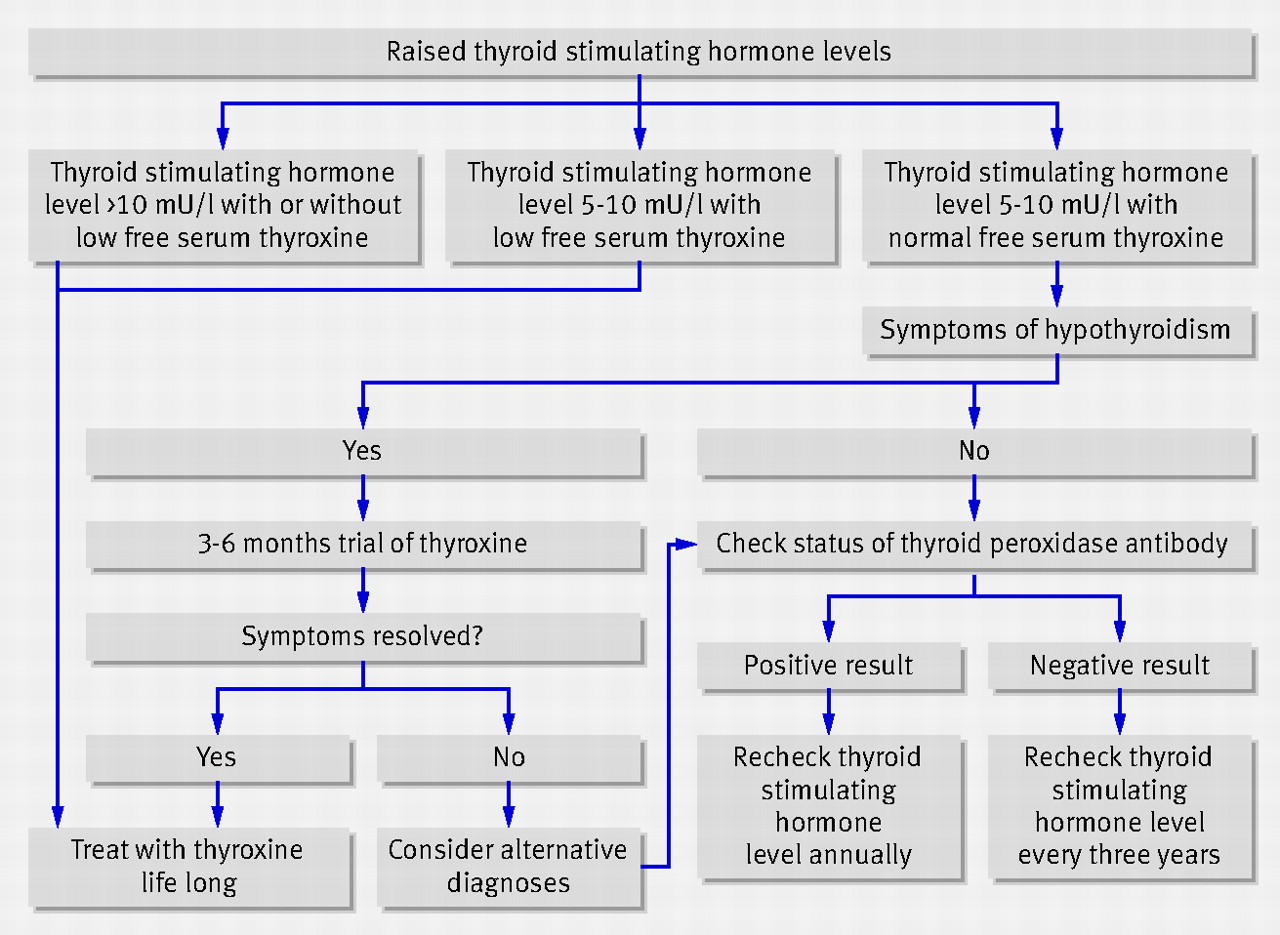
🧪 When to Treat Subclinical Hypothyroidism
- TSH ≥10 mIU/L on 2 occasions → levothyroxine
- TSH 4–10 + symptoms → consider 6-month trial; stop if no benefit
💊 Treatment
- First-line: Levothyroxine (T4) monotherapy
- Starting dose: Adults ~50–100 mcg OD; elderly/IHD 25–50 mcg OD → titrate slowly ⬆️
- Take consistently; avoid interaction with iron, calcium, GI disorders
- T3 (liothyronine) rarely used; specialist only
- Central hypothyroidism: titrate using FT4
- Pregnancy: increase dose 25–50%, monitor TSH/FT4 closely 🤰
📈 Monitoring (NICE NG145)
- Primary: TSH every 6–8 weeks until stable → annual
- Persistent symptoms with normal TSH → check FT4
- Central: monitor FT4, TSH unreliable
🚨 Emergencies & Referral
- Myxoedema coma ❄️🛌 → ICU/HDU, IV thyroid hormone + IV hydrocortisone
- Referral: pregnancy, <16y, pituitary disease, difficult TFTs, cardiac disease, drug interactions
📉 ECG Findings
🧪 Treatment Algorithm
🧾 Clinical Cases
Case 1 – Overt primary hypothyroidism 👩🦰
32F, fatigue, weight gain, constipation, cold intolerance. TSH 18, FT4 low, TPO Ab +.
👉 Management: start levothyroxine; recheck TSH ~3 monthly until stable, then annual.
Case 2 – Older patient with IHD ❤️
75M, lethargy, bradycardia, TSH 12, FT4 low.
👉 Management: start low-dose levothyroxine 25–50 mcg OD, titrate slowly, monitor for angina/arrhythmia.
Case 3 – Subclinical hypothyroidism 🧪
48M, tiredness, TSH 6.8, FT4 normal.
👉 Next step: repeat TFTs in 3–6 months, check TPO Ab.
👉 Management: trial of levothyroxine if symptoms persist; start if TSH ≥10.