
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Spinal Cord
Related Subjects: |Transverse myelitis |Acute Disseminated Encephalomyelitis |Cervical spondylosis |Spinal Cord Anatomy |Acute Disc Prolapse |Spinal Cord Compression |Spinal Cord Haematoma |Foix-Alajouanine syndrome |Cauda Equina |Conus Medullaris syndrome |Anterior Spinal Cord syndrome |Central Spinal Cord syndrome |Brown-Sequard Spinal Cord syndrome |Internal Decapitation
🛑 Trauma safety first: In head injury, reduced consciousness, intoxication, or distracting injuries, assume a cervical spine injury until proven otherwise. Use manual in-line stabilisation and a correctly sized collar if appropriate, and ensure imaging adequately visualises the C7/T1 junction (common “missed” level). Early recognition matters because secondary cord injury (hypoxia, hypotension, swelling) is often preventable. ⚠️
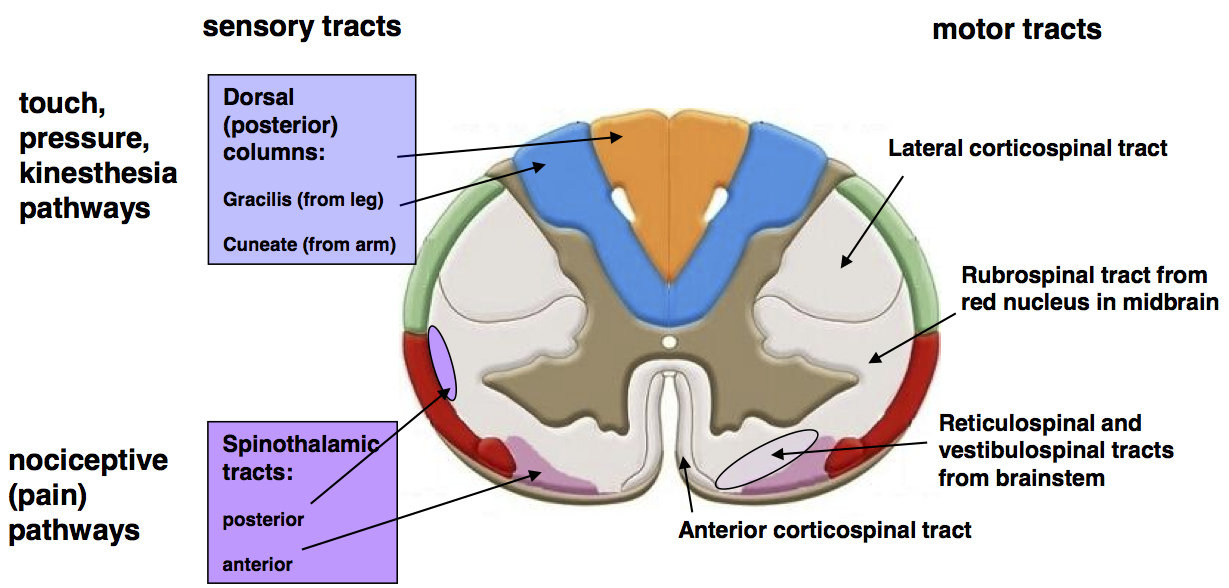
Figure 1: Overview of spinal cord levels and spinal nerve regions.
📍 1) Overview: what the spinal cord is and where it sits
- Definition: The spinal cord is part of the CNS, acting as a signal highway between brain and body, and as a reflex centre.
- Extent: From the foramen magnum (continuous with medulla) to around L1–L2 in adults.
- Below L1–L2: The canal contains the cauda equina (lumbar/sacral nerve roots) and filum terminale.
- Enlargements: Cervical (upper limb) and lumbosacral (lower limb) enlargements reflect higher motor/sensory demand.
- High-yield function levels:
- 🫁 C3–C5 = phrenic nerve → diaphragm (“C3,4,5 keep the diaphragm alive”).
- 🦾 C5–T1 = brachial plexus → upper limb motor/sensation.
- 🚶 L2–S2 = major lower limb motor/sensation.
- 🚽 S2–S4 = bladder/bowel/sexual function (“S2,3,4 keep the pelvic floor”).
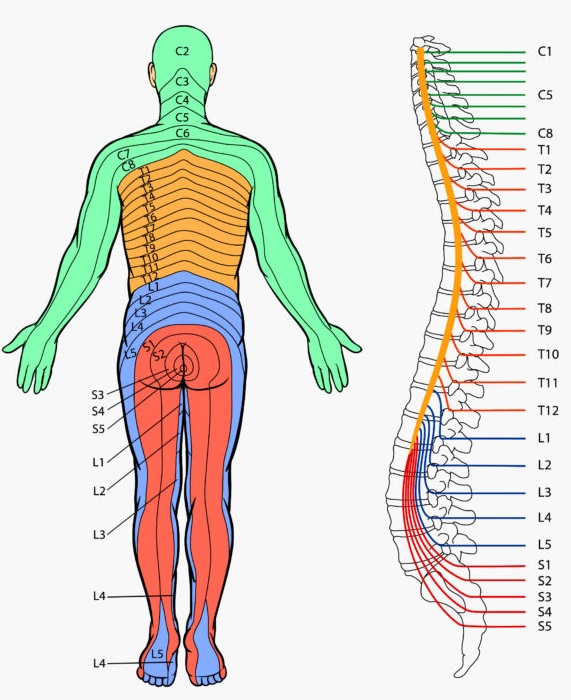
🧩 2) Spinal nerves, roots, and dermatomes (the wiring)
- 31 pairs of spinal nerves:
- Cervical: 8 (C1–C8)
- Thoracic: 12 (T1–T12)
- Lumbar: 5 (L1–L5)
- Sacral: 5 (S1–S5)
- Coccygeal: 1 (Co1)
- Dorsal (posterior) root = sensory afferents; contains a dorsal root ganglion (cell bodies).
- Ventral (anterior) root = motor efferents (and autonomics).
- Roots join → mixed spinal nerve → exits via intervertebral foramen → divides into rami.
- Numbering: C1 exits above C1 vertebra; C8 exits between C7/T1; thereafter nerves exit below their vertebra.
🏗️ 3) Protective layers and spaces (why LP works)
- Meninges: dura mater (tough outer), arachnoid mater, pia mater (adherent).
- CSF lies in the subarachnoid space (between arachnoid and pia).
- Epidural space (outside dura) contains fat and venous plexus → target for epidural anaesthesia.
- Clinical: Lumbar puncture is performed below cord termination (typically L3/4 or L4/5) to avoid cord injury.
🧠 4) Internal spinal cord structure (grey vs white matter)
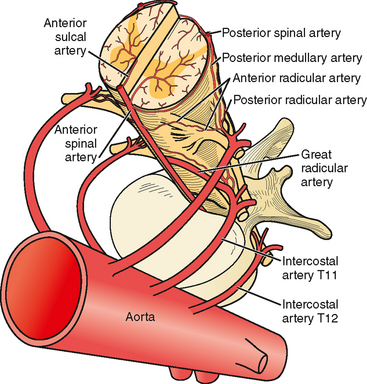
Figure 2: Cross-section showing grey matter horns and surrounding white matter tracts.
- Grey matter (central “butterfly”):
- Dorsal horn 🧊 = sensory processing (pain, temperature, touch input).
- Ventral horn 💪 = lower motor neurons → skeletal muscle.
- Lateral horn ⚡ = autonomics:
- T1–L2 = sympathetic preganglionics.
- S2–S4 = parasympathetic outflow (pelvic splanchnics).
- White matter (outer):
- Myelinated axons arranged into ascending (sensory) and descending (motor) tracts.
- Organised into dorsal, lateral, and anterior funiculi.
🛤️ 5) Major ascending and descending tracts (exam + bedside localisation)
🧭 Localisation shortcut: Dorsal columns = vibration/proprioception; Spinothalamic = pain/temperature; Corticospinal = motor strength. Their crossing patterns explain classic syndromes like Brown-Séquard and anterior cord syndrome.
- ⬆️ Dorsal column–medial lemniscus (DCML): fine touch, vibration, proprioception.
- Ascends ipsilaterally in cord (gracilis = legs medial, cuneatus = arms lateral).
- Crosses in the medulla.
- ⬆️ Spinothalamic tract (anterolateral system): pain & temperature (lateral), crude touch (anterior).
- Crosses within ~1–2 segments via the anterior white commissure.
- Then ascends contralaterally.
- ⬇️ Corticospinal tract: voluntary motor control.
- Most fibres cross at the pyramidal decussation in the medulla → lateral corticospinal tract.
- Lesion in cord → ipsilateral UMN signs below the level (spasticity, hyperreflexia, Babinski).
- ⬆️ Spinocerebellar pathways: unconscious proprioception for coordination and posture (clinically: ataxia when disrupted).
🩸 6) Vascular supply (why anterior cord syndrome happens)
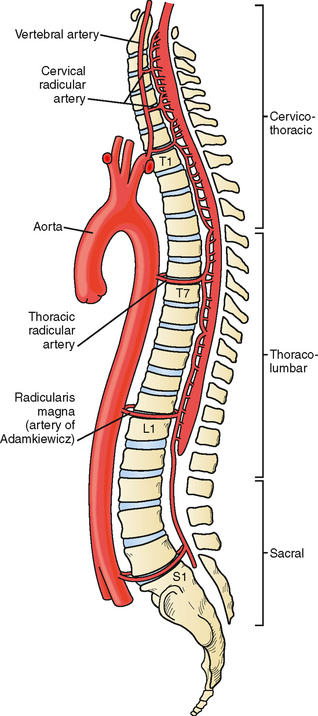
Figure 3: Anterior spinal artery and paired posterior spinal arteries with segmental reinforcement.
- Anterior spinal artery (ASA) = supplies anterior 2/3 (motor tracts, spinothalamic).
- Posterior spinal arteries (paired) = supply posterior 1/3 (dorsal columns).
- Segmental medullary arteries reinforce flow; the largest is the artery of Adamkiewicz (commonly T9–L2 region, variable).
- Watershed risk: Mid-thoracic cord has relatively vulnerable perfusion → hypotension can precipitate ischaemia.
⚙️ 7) Core physiology: what the spinal cord actually does
- Signal conduction: fast myelinated pathways transmit sensory input up and motor output down.
- Reflex arcs: rapid, stereotyped responses without cortical involvement:
- 🧷 Stretch reflex (e.g., knee jerk): muscle spindle → dorsal root → ventral horn → muscle contraction.
- 🔥 Withdrawal reflex: nociceptor input → interneurons → flexor activation + crossed extensor support.
- Autonomic integration: sympathetic outflow (T1–L2) and parasympathetic pelvic control (S2–S4) coordinate:
- BP/HR tone, sweating, thermoregulation
- bladder filling/voiding, bowel motility
- sexual function
🚨 8) Key clinical syndromes (with tract logic)
- 🧊 Spinal shock (early): flaccid weakness + areflexia below lesion, urinary retention. Can last days–weeks.
- ⚡ After shock resolves: UMN features emerge below lesion → spasticity, hyperreflexia, clonus, extensor plantar.
- 🌓 Brown-Séquard (hemicord):
- Ipsilateral motor weakness (corticospinal) below lesion
- Ipsilateral loss of vibration/proprioception (DCML) below lesion
- Contralateral pain/temperature loss (spinothalamic) starting ~1–2 segments below
- 🩸 Anterior cord syndrome (ASA territory):
- Bilateral motor weakness + loss of pain/temperature
- Preserved vibration/proprioception (posterior columns spared)
- 🎯 Central cord syndrome:
- Upper limb weakness > lower limb weakness (classically hyperextension injury + cervical spondylosis)
- Variable sensory loss; may affect bladder
- 🐴 Cauda equina syndrome (LMN root compression):
- Severe back pain ± bilateral sciatica
- Saddle anaesthesia, reduced anal tone
- Urinary retention/incontinence, sexual dysfunction
- LMN weakness/areflexia → surgical emergency
🧪 9) Assessment and investigations (practical UK approach)
- Primary survey: ABCDE + spinal precautions in trauma.
- Neuro exam: motor power, dermatomal sensation, reflexes, tone, perianal sensation and PR tone if CES suspected.
- Imaging:
- CT = best for bony injury in trauma (cervical spine CT often first-line in significant mechanisms).
- MRI = best for cord, discs, ligaments, haematoma, and compressive lesions.
- Red flags: progressive weakness, sensory level, sphincter symptoms, saddle anaesthesia → urgent MRI and specialist review.
🛠️ 10) Management principles (what prevents secondary injury)
🎯 The “secondary hit” is often avoidable: hypoxia and hypotension worsen cord ischaemia and swelling. So early management focuses on airway/oxygenation, haemodynamic support, immobilisation, and rapid imaging/surgical decompression when indicated.
- Immobilisation: manual in-line stabilisation, collar/vacuum mattress as appropriate, careful transfers.
- Perfusion: treat shock aggressively; avoid hypotension (cord perfusion is pressure-dependent).
- Respiratory support: high cervical injuries may require ventilation (C3–C5 involvement threatens diaphragm).
- Definitive care: urgent neurosurgery/orthopaedics for decompression and stabilisation when unstable or compressed.
- Complication prevention: pressure area care, VTE prophylaxis, bladder/bowel plan, early rehab.
📊 Quick tables: key neuro levels (high yield)
| Level | Motor (key) | Sensation (key landmark) | Reflex |
|---|---|---|---|
| C5 | Deltoid / shoulder abduction | Lateral upper arm | Biceps (C5–C6) |
| C6 | Wrist extension | Thumb / lateral forearm | Brachioradialis (C5–C6) |
| C7 | Elbow extension | Middle finger | Triceps (C7–C8) |
| L3 | Knee extension | Medial knee/anterior thigh | Patellar (L3–L4) |
| L4 | Ankle dorsiflexion | Medial shin/foot | Patellar (L3–L4) |
| S1 | Ankle plantarflexion | Lateral foot | Achilles (S1–S2) |
| S2–S4 | Pelvic floor | Saddle area | Anal wink/bulbocavernosus |
✅ Summary
The spinal cord is a conduit, a reflex processor, and an autonomic controller. Understanding tract anatomy (DCML vs spinothalamic vs corticospinal), blood supply (ASA vs posterior arteries), and segmental levels allows rapid bedside localisation and safer emergency management. Clinically, protecting airway/oxygenation, maintaining perfusion, and early imaging/decompression are key to preventing secondary neurological loss. 🧠🛡️
📚 References (UK-focused)
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery