
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Cushing syndrome
⚠️ Important: Hypokalaemia is more likely when the source of ACTH is malignant. 🧠 A normal pituitary MRI does not exclude Cushing’s disease – up to 50% (especially children) may have normal imaging. 👉 In such cases, inferior petrosal sinus sampling is crucial.
📖 About
- Cushing's Syndrome = chronic exposure to excessive cortisol.
- Disrupts hypothalamic–pituitary–adrenal (HPA) axis feedback 🔄.
- Loss of normal circadian cortisol rhythm 🌙☀️.
- Cushing’s Disease = pituitary adenoma secreting ACTH.
🧬 Aetiology
- 🌟 ACTH-dependent:
- 🧠 Pituitary adenoma (Cushing’s disease).
- 🫁 Ectopic ACTH from tumours (e.g. lung, pancreas).
- 🌟 ACTH-independent:
- 🟤 Adrenal adenomas/carcinomas.
- 💊 Exogenous glucocorticoids (most common overall cause).
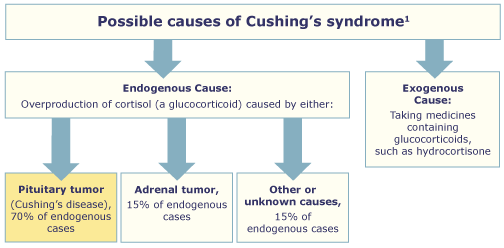
⚡ Causes
- 🧠 Pituitary Adenoma (Cushing’s Disease) (~70% endogenous)
- Microadenomas → ↑ACTH → bilateral adrenal hyperplasia.
- Key: not suppressed by low-dose dex, partially suppressed by high-dose; ↑ACTH & cortisol; responds to CRH.
- 🟤 Adrenal Tumours
- Autonomous cortisol secretion → suppressed ACTH.
- No suppression on low or high-dose dex.
- 🫁 Ectopic ACTH Production
- Sources: small cell lung carcinoma, bronchial carcinoid, pancreatic NET.
- ACTH high, no suppression on high-dose dex.
- Often severe hypokalaemia ⚠️ due to mineralocorticoid activity.
- 💊 Iatrogenic – long-term glucocorticoid therapy (asthma, RA, PMR, UC, post-transplant).
- 🎭 Pseudo-Cushing’s – alcohol excess, severe obesity, depression (reversible).
- 🤰 Pregnancy – ↑ cortisol-binding globulin → raised total cortisol (rarely true Cushing’s).
👀 Clinical Features
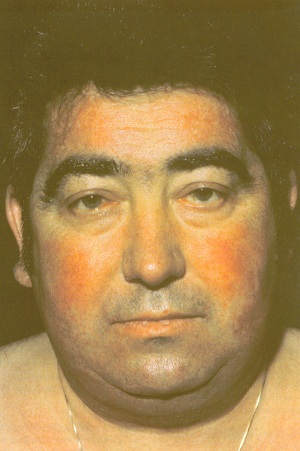
- Appearance 🌙:
- Centripetal obesity.
- Moon face, facial plethora, acne.
- Dorsocervical fat pad (“buffalo hump”).
- Muscle wasting → thin extremities.
- Purple striae (abdomen, thighs, breasts).
- Skin 🩹:
- Thin fragile skin, easy bruising.
- Slow wound healing.
- Hirsutism in women.
- Hyperpigmentation (if ACTH-driven).
- MSK 💪:
- Proximal myopathy (difficulty standing/climbing stairs).
- Osteoporosis → fractures.
- Avascular necrosis of femoral head.
- Metabolic 🧪:
- Glucose intolerance / diabetes.
- Hyperlipidaemia.
- Hypertension.
- Hypokalaemia & metabolic alkalosis.
- Neuropsychiatric 🧠:
- Mood swings, depression, psychosis.
- Cognitive impairment.
- Reproductive ❤️:
- Women: amenorrhoea, infertility.
- Men: ↓ libido, impotence.
- Growth 📏:
- Stunted growth in children.
- Immune 🛡️:
- Infections, reactivation of TB.
- Poor wound healing.


🧪 Diagnostic Tests
🌙 Overnight Dexamethasone Suppression (screen)
- 1 mg dex at midnight → cortisol at 08:00.
- Normal < 50 nmol/L;> 50 → suspect Cushing’s.
- ⚠️ False positives: depression, obesity, alcohol, phenytoin.
🧪 24h Urinary Free Cortisol (screen)
- Normal < 280 nmol/24h; elevated = abnormal.
💉 Low-Dose 48h Dex Test (confirm)
- 0.5 mg dex 6-hourly × 48h (total 4 mg).
- Cortisol undetectable = excludes; detectable = Cushing’s confirmed.
📊 High-Dose 48h Dex Test (localise)
- 2 mg dex 6-hourly × 48h (total 16 mg).
- Pituitary: >50% suppression.
- Ectopic/adrenal: no suppression.
🧬 Plasma ACTH
- ⬇️ Undetectable → adrenal tumour.
- ⬆️ High → pituitary vs ectopic.
- CRH test: rise = pituitary; no rise = ectopic.
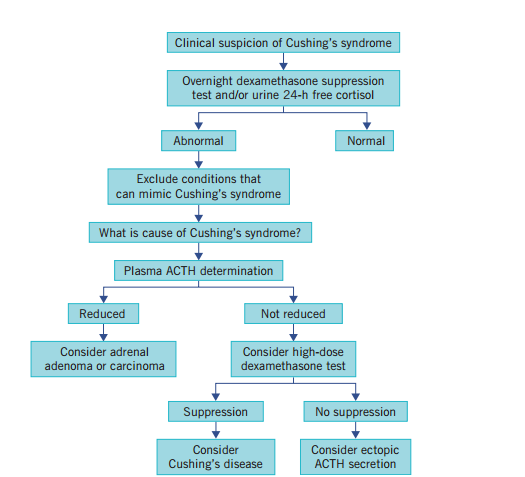
📚 Exam Tip: Think stepwise → Overnight (screen) → Low-dose (confirm) → High-dose/ACTH (localise). Pituitary = suppressible, ectopic/adrenal = resistant.
🖼️ Imaging
- 🧠 Pituitary MRI (but 50% normal!) → may need inferior petrosal sinus sampling.
- 🟤 Adrenal CT/MRI → adenoma or carcinoma.
- 🫁 Chest/abdomen CT → ectopic ACTH tumours.
- 📡 Octreotide scans for ectopic localisation.
💊 Management
- 🧠 Pituitary adenoma: transsphenoidal resection; radiotherapy if unsuccessful; pasireotide or ketoconazole if refractory.
- 🟤 Adrenal tumours: adrenalectomy ± mitotane if carcinoma.
- 🫁 Ectopic ACTH: treat primary tumour if resectable; otherwise medical control of cortisol.
- 💊 Iatrogenic: gradual steroid taper, switch to steroid-sparing alternatives.
🧪 Medical Therapy (for inoperable / pre-surgery)
- Metyrapone (11β-hydroxylase inhibitor).
- Ketoconazole (blocks steroidogenesis).
- Aminoglutethimide (cholesterol → pregnenolone block).
- Mitotane (adrenolytic, carcinomas).
- Etomidate (IV emergency use).
📌 Key Points
- Early recognition prevents morbidity & mortality.
- Diagnosis = stepwise biochemical + imaging + sometimes petrosal sampling.
- Management is cause-directed (surgery first-line where possible).
- 🏥 Long-term follow-up essential: recurrence, metabolic complications, bone health, psychological support.
Cases - Cushing’s Syndrome
- Case 1 - Iatrogenic steroid use 💊: A 55-year-old woman with rheumatoid arthritis on long-term prednisolone presents with weight gain, easy bruising, proximal muscle weakness, and thin skin. Exam: moon facies, buffalo hump, purple abdominal striae. Diagnosis: exogenous Cushing’s syndrome due to chronic glucocorticoid therapy. Managed by gradual tapering of steroids and use of steroid-sparing agents.
- Case 2 - Pituitary-dependent (Cushing’s disease) 🧠: A 36-year-old woman presents with irregular menses, hirsutism, and worsening acne. Exam: central obesity, hypertension, and skin thinning. Bloods: elevated cortisol not suppressed by low-dose dexamethasone, but suppressed with high-dose dexamethasone. MRI: pituitary microadenoma. Diagnosis: Cushing’s disease (ACTH-secreting pituitary adenoma). Managed with trans-sphenoidal pituitary surgery.
- Case 3 - Adrenal tumour ⚠️: A 42-year-old man presents with new-onset diabetes, hypertension, and muscle wasting. No exogenous steroid use. Bloods: raised cortisol with suppressed ACTH. CT abdomen: adrenal mass. Diagnosis: ACTH-independent Cushing’s syndrome due to adrenal adenoma. Managed with adrenalectomy.
Teaching Point 🩺: Cushing’s syndrome = chronic glucocorticoid excess. Common causes: exogenous steroids, pituitary adenoma (Cushing’s disease), adrenal adenoma/carcinoma, ectopic ACTH (e.g. small-cell lung cancer). Clinical clues: central obesity, moon facies, striae, proximal weakness, hypertension, diabetes, mood changes. Diagnosis: screen with 24h urinary cortisol, overnight dexamethasone suppression, late-night salivary cortisol. Management: treat underlying cause (taper steroids, pituitary surgery, adrenalectomy).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery