Related Subjects:
|ECG Basics
|ECG Axis
|ECG Analysis
|ECG LAD
|ECG RAD
|ECG Low voltage
|ECG Pathological Q waves
|ECG ST/T wave changes
|ECG LBBB
|ECG RBBB
|ECG short PR
|ECG Heart Block
|ECG Asystole and P wave asystole
|ECG QRS complex
|ECG ST segment
|ECG: QT interval
|ECG: LVH
|ECG RVH
|ECG: Bundle branch blocks
|ECG Dominant R wave in V1
|ECG Acute Coronary Syndrome
|ECG Crib sheets
💔 Victims of sudden cardiac arrest presenting with asystole have an extremely poor prognosis.
📊 Around 10% survive to admission; only 0–2% survive to hospital discharge.
📖 About
- ⚡ Asystole accounts for ~40% of cardiac arrests.
- 🪫 It represents the terminal rhythm in most cases of cardiac arrest.
🦠 Aetiology
- ⏱️ Usually arises from prolonged untreated ventricular fibrillation.
- ⚡ May occur after unsuccessful defibrillation of VF/VT.
- Can follow profound hypoxia, massive haemorrhage, or metabolic derangements.
🔍 Clinical
- GCS 3, no pulse, not breathing.
- Telemetry/monitor: flat line tracing.
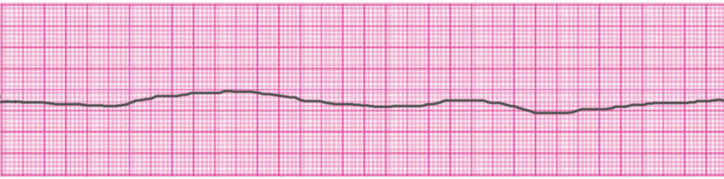
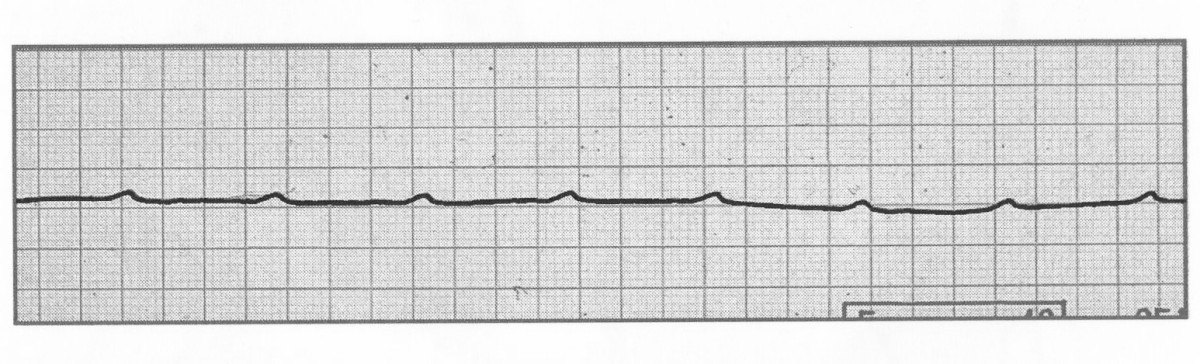
📉 ECG
- 📏 Rate: No ventricular activity (occasionally ≤6/min). “P-wave asystole” may occur with isolated atrial activity but absent QRS.
- 📏 Rhythm: No organised ventricular activity.
- ⛔ PR/QRS: Cannot be determined; no QRS complexes present.
⚠️ Differentials
- 🎛️ Check monitor/lead placement - exclude fine VF.
🚑 Management (UK Resus Council/ALS)
- 🔄 Immediate actions: Start CPR, give high-flow oxygen, apply monitoring/defibrillator pads.
- 💉 Secure IV/IO access.
- 💊 Adrenaline (epinephrine): 1 mg IV/IO every 3–5 minutes.
- ⚡ Not shockable: Defibrillation is not indicated unless rhythm changes to VF/VT.
- 🔍 Confirm asystole in ≥2 leads before decisions about terminating resuscitation.
- 🚫 Atropine is no longer recommended in asystole (AHA/ERC guidelines).
🛑 Reversible Causes (“4 Hs & 4 Ts”)
- 💧 Hypovolaemia – IV fluids, transfusion if bleeding.
- 🌬️ Hypoxia – 100% O₂, airway check, suction, confirm tube position.
- 🧪 Hydrogen ion (acidosis) – optimise ventilation; consider bicarbonate if severe.
- ⚡ Hypo/hyperkalaemia – give potassium (if low); if high, treat with calcium chloride + insulin/dextrose ± sodium bicarbonate.
- ❄️ Hypothermia – active rewarming, warmed IV fluids.
- 🫁 Tension pneumothorax – needle decompression then chest drain.
- ❤️ Cardiac tamponade – ultrasound, pericardiocentesis.
- 🧴 Toxins – consider overdose, stop infusions, antidotes as available.
- 🩸 Thrombosis (coronary/pulmonary) – consider thrombolysis, PCI, or thrombectomy if appropriate.
📚 References
📝 Revision Notes
- 📌 Asystole = non-shockable. Immediate CPR + adrenaline are the only evidence-based interventions.
- 📌 Always exclude fine VF or equipment error before labelling a rhythm asystole.
- 📌 Survival depends on rapidly identifying and reversing an underlying cause.
