
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Moyamoya disease
Related Subjects: |Subarachnoid Haemorrhage |Haemorrhagic stroke
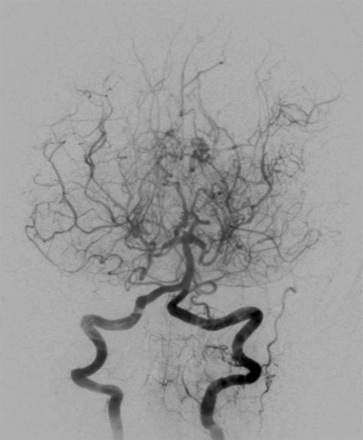
🌫️ Moyamoya disease is a progressive, non-inflammatory vasculopathy affecting the intracranial internal carotid arteries (ICA), middle cerebral arteries (MCA), and anterior cerebral arteries (ACA). It causes both ischaemic and haemorrhagic stroke. On angiography, a hazy network of collateral vessels forms, resembling "moyamoya" - the Japanese word for smoke drifting in the air. First described in 1957, the name was popularised by Jiro Suzuki in 1965 and later codified [Suzuki J, 1983].
📖 About
- Described in Japan in 1957 as “hypoplasia of the bilateral ICAs”; renamed “Moyamoya” in 1965.
- 🧮 Incidence: ~10/100,000 in Japan; ~1/1,000,000 in the USA.
- Involves progressive ICA occlusion and development of fragile collateral vessels.
- Increased basic fibroblast growth factor has been implicated in pathogenesis.
- Can be sporadic or familial, leading to both ischaemic and haemorrhagic stroke.
🧬 Genetics
- Most common in Japanese, Chinese, and Korean populations (10x more frequent than in Europeans).
- Familial clustering: linked to variants on chromosome 17 (e.g., RNF213 gene).
- Seen worldwide, including non-Asian cohorts.
⚙️ Aetiology & Pathophysiology
- Affects the distal ICA, MCA, and ACA stems.
- Results in extensive collateralisation via lenticulostriate, thalamic, and transdural anastomoses.
- Non-inflammatory; pathology shows intimal hyperplasia with lumen narrowing.
- Fragile collaterals predispose to haemorrhage.
- Similar angiographic patterns (“Moyamoya syndrome”) may occur with atherosclerosis, diabetes, or sickle cell disease.
🤝 Associations
- Haematological: Sickle cell disease, β-thalassaemia, hereditary spherocytosis, Fanconi anaemia.
- Neurological/genetic: Neurofibromatosis type 1.
- Metabolic/immune: Homocystinuria, antiphospholipid syndrome, Grave’s disease, SLE.
🩺 Clinical Presentation
- Common in children/young adults, but may present at any age.
- ⛔ Ischaemic events: recurrent hemiplegia, TIAs, cognitive impairment, silent infarcts.
- ⚡ Seizures and movement disorders (chorea, dystonia) may occur.
- 💥 Haemorrhage: intraparenchymal or intraventricular bleed from fragile collaterals.
🔍 Investigations
- 🧪 Bloods: Usually normal; confirms non-inflammatory nature.
- 🖼️ CT: Cortical/subcortical infarcts, volume loss, haemorrhage.
- 🧲 MRI/MRA: Gold standard → ICA narrowing + “puff of smoke” collaterals. FLAIR: “Ivy sign” from slow cortical flow. GRE: Detects microhaemorrhages in basal ganglia/thalamus.
- 📡 Transcranial Doppler: Non-invasive assessment of stenosis/hemodynamics.
- ⚡ EEG: In children → “re-build-up phenomenon” after hyperventilation.
- 🩻 Perfusion imaging: Identifies hypoperfused territories at risk of infarct.
📊 Suzuki Angiographic Stages
- 1️⃣ Early ICA stenosis.
- 2️⃣ Development of Moyamoya collaterals at brain base.
- 3️⃣ Progressive ICA occlusion; ↑ collateral vessels, ↓ MCA/ACA flow.
- 4️⃣ Circle of Willis + PCA occlusion; extracranial–intracranial collateralisation.
- 5️⃣ Fewer Moyamoya vessels; major arteries absent.
- 6️⃣ Disappearance of Moyamoya collaterals; brain perfused only by ECA branches.
⚖️ Management
- Best managed in specialist neurosurgical centres.
- 📉 Medical therapy: Limited role. BP optimisation crucial. Antiplatelets are sometimes used in children but avoided in adults due to haemorrhage risk.
- 🧑⚕️ Surgical revascularisation: - Direct bypass: STA–MCA anastomosis. - Indirect: Encephaloduroarteriosynangiosis (EDAS), burr holes, encephalomyosynangiosis (EMS). Recent studies show direct bypass reduces haemorrhagic risk most effectively.
- 💊 Aspirin often used in children; usually stopped in adults due to bleed risk.
- 📉 Most common cause of death: haemorrhage from fragile collaterals.
📖 Further Reading
- Moyamoya Disease and Syndrome - NEJM, 2009
- Treatment and Outcomes in Moyamoya - J Stroke, 2016
- EEG findings in childhood Moyamoya - Neurosurg Rev, 1992
- MRI vs CT perfusion in Moyamoya - Sichuan Univ J Med, 2018
- Multiple burr hole surgery - Acta Neurochir, 2018
💡 Exam Pearl: Moyamoya = young patient + recurrent TIAs/strokes + angiogram “puff of smoke.” Think early referral for surgical revascularisation to prevent ischaemia and haemorrhage.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery