Related Subjects:
|Neurological History taking
|Cortical functions
|Motor System
|Sensory System
|Mental state Examination
|Speech and Language Exam
|Cranial nerves and examination
|Assessing Cognition
🧠 Neurological diagnosis relies ~90% on a good history, supported by examination, imaging, and investigations. Establish a clear timeline and pattern of evolution of symptoms.
🧭 Five-Step Approach
- 📍 Location: Where is the lesion? Use history + neuroanatomy.
- 🧬 Causation: What is it? Think onset speed, periodicity, risk factors, age.
- 📑 Confirmation: Imaging, neurophysiology, genetics – only when it adds value.
- 💬 Explanation: Clear communication with the patient and family.
- 💊 Treatment: Decide if treatable, untreatable, or high-risk (e.g., surgical danger).
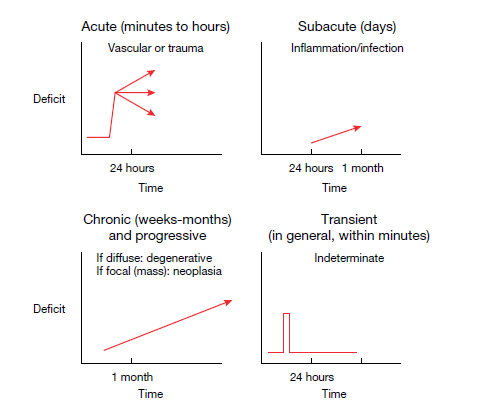
⏱️ Symptom Timings & Periodicity
- Seconds–Minutes: Stroke/TIA/SAH (🛑 negative signs), seizures (⚡ positive signs).
- Hours–Days: Inflammatory (MS, ADEM), infections (meningitis, encephalitis).
- Weeks–Months: Tumours 🎗️, MND, CJD, subacute combined degeneration.
- Months–Years: Alzheimer’s, Parkinson’s, slow-growing tumours (e.g. meningioma).
🔄 Patterns
- ⏳ Transient & recurrent: TIA, epilepsy.
- 💥 Sudden worst onset → gradual recovery: Stroke, MS relapse.
- 🌙 Diurnal:
- Myasthenia → worse as day progresses.
- Raised ICP → headache worse on waking.
- 📅 Relapsing-remitting: MS.
🧩 Levels of Damage
🧠 Cortical
- Functional disorders (real, not malingering) – need empathy.
- Right cortex → left weakness ± cortical signs: dysphasia, neglect, apraxia.
- Internal capsule → pure motor/sensory deficit, no cortical signs.
⚙️ Subcortical
- Basal ganglia: Parkinsonism, chorea, hemiballismus.
- Thalamus: Sensory integration loss, thalamic pain, amnesia.
🚦 Brainstem
- “Crossed signs” = ipsilateral CN palsy + contralateral motor/sensory deficit.
- Midbrain: CN III/IV, red nucleus, substantia nigra.
- Pons: CN V–VIII, cerebellar connections.
- Medulla: CN IX–XII, corticospinal decussation.
🎯 Cerebellum
- Lateral → ipsilateral limb incoordination.
- Midline/vermis → truncal ataxia.
🦴 Spinal Cord
- Above C5–T1 → quadriplegia.
- Below T1 → paraplegia.
- Syndromes depend on tract involvement (DCML, spinothalamic, corticospinal).
🐎 Cauda Equina
- LMN weakness, saddle anaesthesia, areflexia, loss of anal tone 🚨.
- Emergency MRI & decompression.
⚡ Anterior Horn Cell
- LMN signs: wasting, fasciculations, weakness. Classic in MND.
🌐 Peripheral Nervous System
- Nerve roots: Dermatomal pain/weakness, reflex loss.
- Peripheral nerves: Glove-and-stocking loss (neuropathy).
- Individual nerves: Predictable mixed motor + sensory loss.
- NMJ: Myasthenia gravis → fatigable weakness, ptosis, diplopia.
- Muscle: Weakness, wasting, pseudohypertrophy (e.g., muscular dystrophies).
