
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Haemoptysis
Related Subjects: |Idiopathic Pulmonary Fibrosis |Diffuse Parenchymal Lung disease |Asbestos Related Lung disease |Sarcoidosis |Coal Worker's Pneumoconiosis |Silicosis |Farmer's Lung |Cryptogenic Organising Pneumonia (COP-BOOP) |Extrinsic Allergic alveolitis (Hypersensitivity) |Byssinosis |Pneumoconiosis |Cor Pulmonale |Chest X Ray Interpretation | Lung Cancer
🫁 Introduction
Haemoptysis = coughing up blood originating from the lower respiratory tract. ⚠️ Massive haemoptysis is a medical emergency → mortality is usually due to asphyxiation rather than blood loss. 💡 As little as 250 mL can fill the bronchial tree and obstruct the airway. 🎯 Always confirm the source (lung vs nasopharynx vs GI tract).
📊 About
- Common causes: TB, bronchiectasis, aspergilloma, lung cancer.
- Lungs have dual blood supply: pulmonary + bronchial arteries.
- 👉 Most haemoptysis originates from the bronchial arterial system (systemic pressure → brisk bleeding).
- Pulmonary circulation can shunt blood away from hypoxic zones.
🦠 Causes
- 🎗️ Malignancy: Bronchogenic carcinoma, metastases (esp. in smokers >40).
- 🦠 Infective: Pneumonia, lung abscess, TB (upper lobe lesions in young).
- 🍄 Aspergilloma: Cavitary disease → classically recurrent haemoptysis.
- 🌪️ Bronchiectasis: Purulent sputum, recurrent infection, CF common.
- 🚨 Trauma: Biopsy, bronchoscopy, penetrating injury.
- 🧬 Vasculitis: GPA (c-ANCA), Goodpasture’s (anti-GBM).
- 🫀 Vascular: PE with infarction, AVMs.
- 💉 Bleeding disorders: Thrombocytopenia, anticoagulation (warfarin, DOACs).
- ❤️ Cardiac: Mitral stenosis → pulmonary venous hypertension.
- 🌀 Other: Autoimmune disease, factitious haemoptysis.
🧑⚕️ Clinical Features
- History: smoking 🚬, TB exposure, weight loss ⚖️, bleeding disorders.
- Massive haemoptysis = >600 mL/24h or rapid bleeding with airway threat.
- Exam: clubbing, cachexia, chest crepitations, signs of chronic lung disease.
- Always distinguish from: – Epistaxis (nasopharyngeal blood trickling) 👃 – Haematemesis (vomiting blood from GI tract) 🍷
🧪 Investigations
- 🩸 Bloods: FBC, U&E, clotting, ABG.
- 🩻 CXR: May show cavitation, mass, consolidation, bronchiectasis.
- 🖥️ CT Angiography: Gold standard for source localisation for any targets for bronchial artery embolisation if stable.
- 👁️ Bronchoscopy: Rigid/flexible to visualise + tamponade bleeding site.
- 🧬 Autoimmune tests: c-ANCA, anti-GBM.
🚨 Management of Massive Haemoptysis
- ABC first! Senior help immediately (respiratory, IR, cardiothoracics).
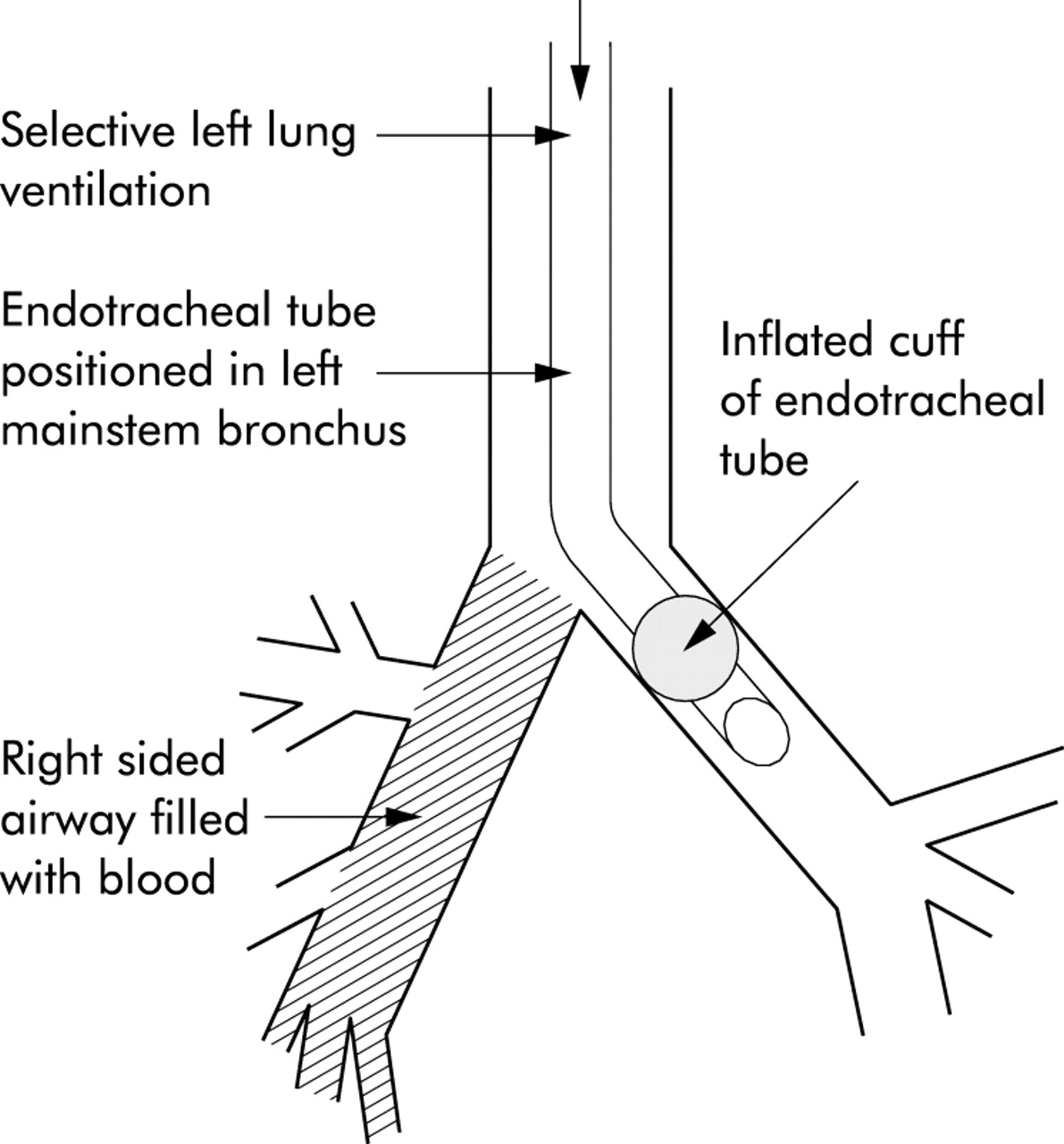
- 🫁 Position: Lie on side of bleeding lung → protect good lung.
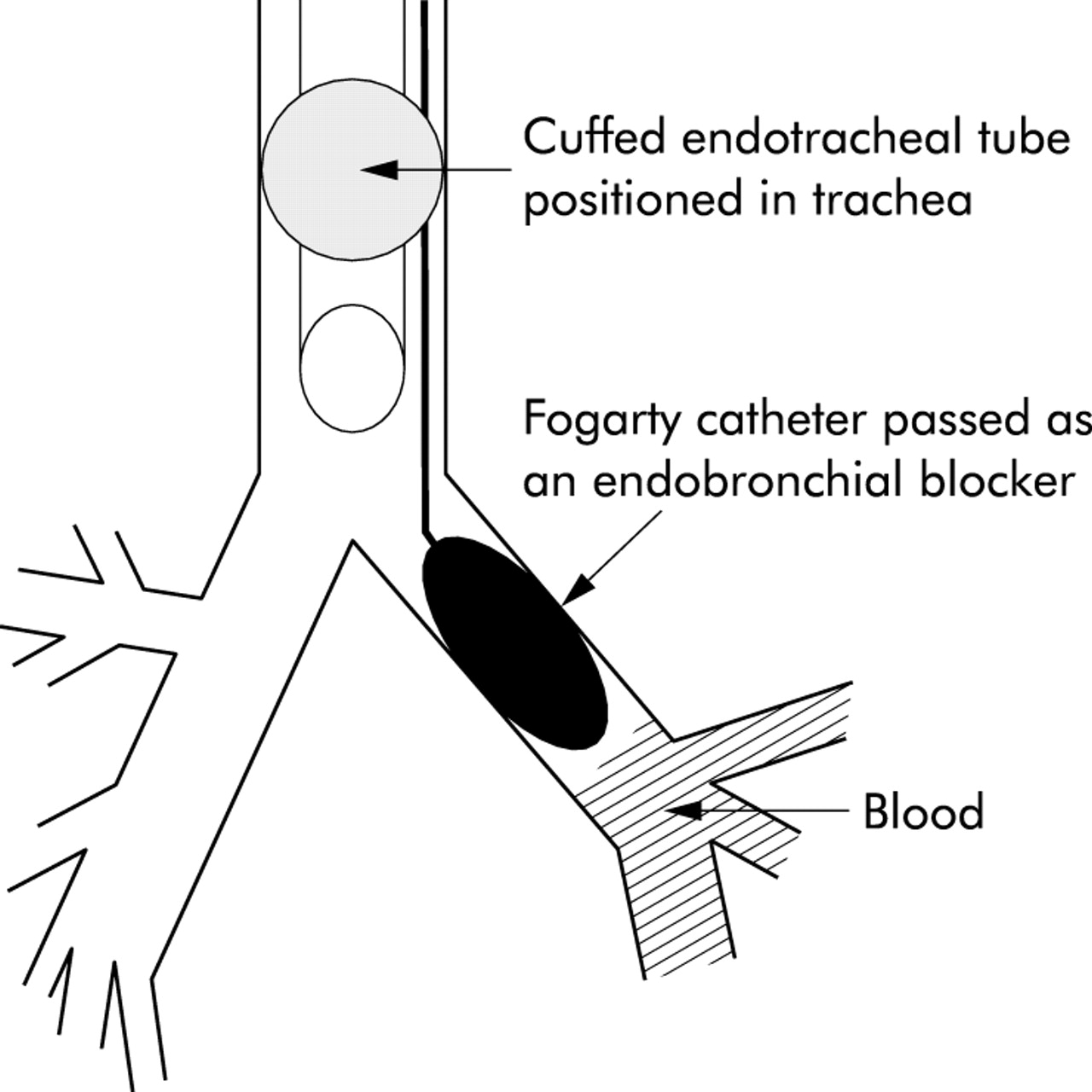
- 💨 Oxygen: High-flow. Intubation if decompensating (selective main bronchus intubation or double-lumen tube).
- 💉 IV Access: Wide-bore cannulae; crossmatch.
- 💊 Drugs:
- Nebulised adrenaline (epinephrine) 5–10 mL of 1:10,000.
- Nebulised tranexamic acid (e.g. 500 mg in 5 mL N-saline) TDS.
- IV tranexamic acid (1 g IV over 10 min, then infusion if needed).
- 🖥️ Imaging: Urgent portable CXR; CT angiography if stable. Use Arterial contrast to Look for bronchial artery embolisation targets
- 🔧 Bronchoscopy: Endobronchial blocker, suction, topical haemostatics.
- 🩻 Interventional Radiology: Bronchial artery embolisation (BAE) = first-line definitive therapy.
- 🔪 Surgery: Lobectomy/pneumonectomy if localised + fit for surgery.
- 🤲 Palliation: In terminal cancer → symptom control (morphine, midazolam, palliative sedation).
📌 Clinical Pearls
- Death in massive haemoptysis = airway obstruction, not blood loss.
- First priority = protect unaffected lung and maintain oxygenation.
- Tranexamic acid is increasingly used (nebulised or IV).
- BAE is highly effective but recurrence is common → monitor long term.
- Always rule out lung cancer in smokers >40 with unexplained haemoptysis.
📚 References
- British Thoracic Society (BTS) Guidelines – Management of Haemoptysis
- BMJ Best Practice: Haemoptysis
- Oxford Handbook of Clinical Medicine
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery