
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Infective Endocarditis
Related Subjects: |Aortic Anatomy |Acute Coronary Syndrome (ACS) General |Aortic Dissection |Acute Heart Failure and Pulmonary Oedema |Aortic Regurgitation (Incompetence) |Aortic Stenosis |Aortic Sclerosis |Transcatheter aortic valve implantation (TAVI) |Infective Endocarditis |Duke’s Criteria for Infective Endocarditis
🩺 The presence of an Endocarditis Team is crucial in IE. This multidisciplinary approach has been shown to significantly reduce 1-year mortality. ⚠️ Do not start antibiotics before taking at least 3 blood cultures over 12+ hrs, using strict aseptic technique.
📖 About
- Infective Endocarditis (IE) = infection of the endocardium and heart valves, usually bacterial.
- Vegetations consist of organisms + fibrin + platelets, may embolise.
- Causes valve destruction, regurgitation, abscesses, and embolic/immune complications.
🧬 Aetiology & Pathophysiology
- Infection of native or prosthetic valves, congenital defects (VSD, bicuspid aortic valve).
- Often seeded by bacteraemia in patients with prior endothelial damage.
- Immune complex deposition → vasculitis, glomerulonephritis, skin signs.
- Emboli may affect brain 🧠, spleen, kidneys, or lungs.
📊 Epidemiology
- Commoner in men
- Increasingly older patients
- IV drug use → right-sided IE (tricuspid valve)
- Underlying rheumatic or congenital heart disease
🦠 Common Organisms
| Organism | Description | Common Situations |
|---|---|---|
| Staphylococcus aureus | Aggressive, acute IE | IVDU, healthcare-associated |
| Streptococcus viridans | Subacute, oral flora | Post-dental procedures |
| Enterococcus spp. | Older adults, subacute | GU or GI procedures |
| Staphylococcus epidermidis | Low-grade, prosthetic valves | PVE esp. <1 yr post-surgery |
| HACEK group | Fastidious GN bacteria | Culture-negative IE |
| Fungal IE | Large vegetations, high mortality | Immunocompromised, IVDU |
⚠️ High Risk Groups
- Prosthetic valve patients (including TAVI)
- Previous IE
- Uncorrected cyanotic congenital heart disease, or within 6 months post-repair
- Cardiac implantable electronic devices (CIEDs)
🩺 Clinical Features
- Constitutional: malaise, fever, sweats, weight loss
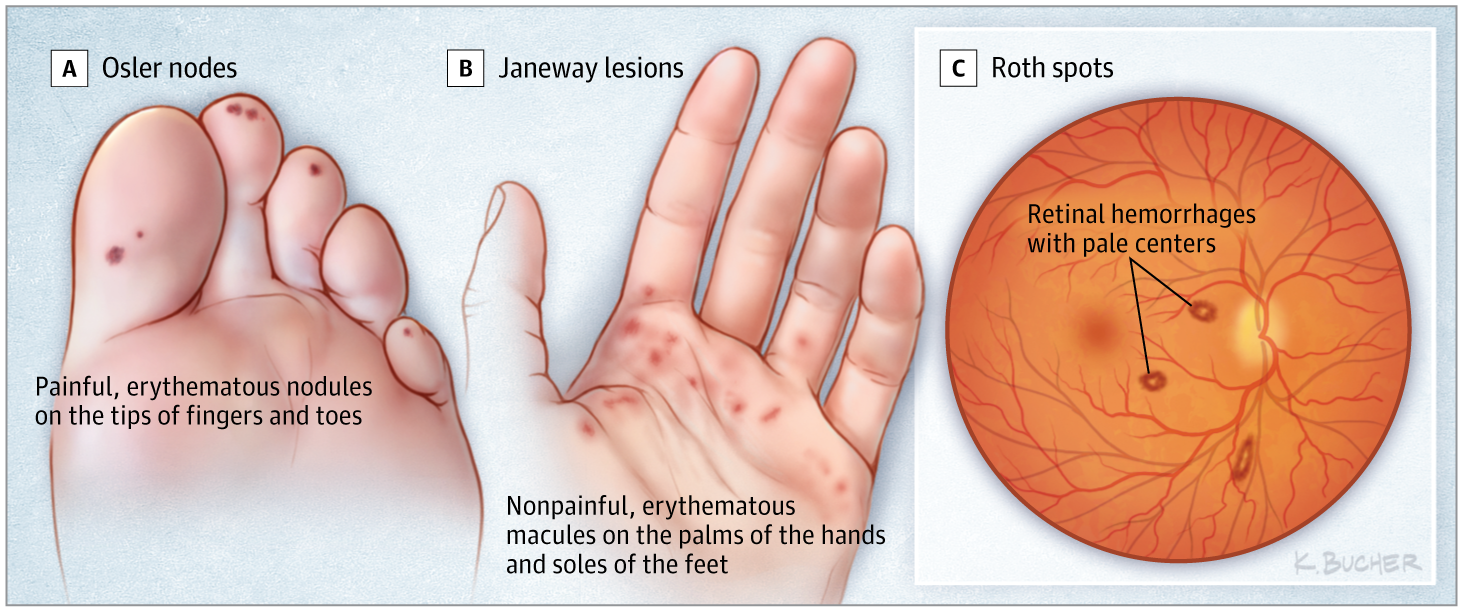
- Osler’s nodes: Tender, peasized nodules on pads of fingers and toes. Often pale in the centre. May occur in crops. Fade after few days usually without breaking down or leaving any residue. Either due to minute emboli in superficial terminal vessels or due to vasculitis.
- Janeway lesions – Large nontender macules on palms and soles, it is vascular phenomenon due to septic embolization.
- Cardiac: new murmur, AF, HF, conduction block
- Embolic: stroke, splenic infarct, lung abscess
- Peripheral stigmata: Roth spots 👁, splinter haemorrhages, Osler nodes (tender), Janeway lesions (painless)
- Right-sided IE → septic lung emboli, cavitating pneumonia
🔍 Diagnosis of Infective Endocarditis (IE) 🫀
The diagnosis of infective endocarditis combines clinical suspicion, microbiology, imaging, and supportive tests. The current standard is the 2023 Duke-ISCVID Criteria - updated to include advanced imaging (PET/CT, cardiac CT), molecular diagnostics, expanded typical organisms, and new risk factors like transcatheter valves and CIEDs.
- Blood cultures: Take ≥3 sets from separate sites before antibiotics whenever possible (unless septic shock or immediate instability) 🩸
- Echocardiography: Start with TTE; escalate to TEE (much more sensitive) for prosthetic valves, devices, poor windows, or suspected abscess/dehiscence 🔎
- Advanced imaging: Use ¹⁸F-FDG PET/CT or cardiac CT as major criteria in difficult/prosthetic cases 📸
- Duke-ISCVID 2023 Criteria: Major + minor criteria → definite, possible, or rejected classification 📊
🫀 The 2023 Duke-ISCVID Criteria improve sensitivity for prosthetic/device IE, culture-negative cases, and modern diagnostics while keeping high specificity ✅
🧪 Pathological Criteria (Definite IE if present) 🔬
- Microorganisms confirmed (culture, histology, PCR, sequencing) from vegetation, valve, abscess, explanted prosthesis/CIED, or embolic material (with active IE signs) 🦠
- Histological evidence of active endocarditis from the above sites 📜
🔑 Major Clinical Criteria 🏆
- Microbiology: Typical IE organisms from ≥2 separate blood cultures; persistently positive with uncommon organisms; positive serology/PCR (Bartonella, Coxiella, etc.) 🧫
- Imaging: Endocardial involvement - vegetation, abscess, new regurgitation, new/prosthetic dehiscence on echo; abnormal uptake on PET/CT; cardiac CT findings; intraoperative confirmation 🌿🩸
⚖️ Minor Criteria 📋
- Predisposing condition: Pre-existing valve lesion/prosthetic/transcatheter valve, CIED, prior IE, IV drug use 💉
- Fever ≥38°C 🌡️
- Vascular phenomena: Major emboli, Janeway lesions, mycotic aneurysm, conjunctival hemorrhage 🩸💥
- Immunological phenomena: Glomerulonephritis, Osler nodes, Roth spots, positive rheumatoid factor 🛡️
- Microbiological evidence not meeting major criteria 🧫
📊 Diagnostic Classification (2023 Duke-ISCVID) 🎯
- Definite IE: Pathological proof OR 2 major OR 1 major + 3 minor OR 5 minor criteria ✅
- Possible IE: 1 major + 1–2 minor OR 3 minor criteria ❓
- Rejected IE: Firm alternative diagnosis OR resolution with <4 days antibiotics (no surgery) OR insufficient evidence ❌
Most Important Investigations 🩺
- Blood cultures: The most critical first step; 3+ sets before antibiotics; identifies typical organisms (viridans strep, S. aureus, enterococci, HACEK, etc.) 🩸🦠
- Echocardiography: TTE first (fast & non-invasive) → TEE if negative but high suspicion, or prosthetic/device present; negative TTE does NOT exclude IE! 📡🔍
- Advanced imaging: PET/CT or CT for perivalvular extension or unclear cases (now major criteria) 📸
Supportive Findings (Helpful clues) 🔍
- Normocytic normochromic anaemia 🩸
- Elevated WBC, CRP (better than ESR for monitoring), ESR 📈
- Microscopic haematuria 🚽
- ECG: New conduction delay / AV block → suspect peri-valvular abscess ⚡🫀
🧪 Practical Diagnostic Approach 🚀
- Suspect IE with fever + new/changing murmur + risk factors (prosthetic valve, IVDU, CIED) or embolic/immunological signs or compatible bacteraemia 🔥🩸
- Get blood cultures BEFORE empiric antibiotics 🩸⏳
- Order TTE → TEE if negative/high suspicion or prosthetic/device present 📡→🔍
- Consider culture-negative IE (prior antibiotics, fastidious organisms) - order serology/PCR 🧪
- Repeat imaging if initial negative but persistent suspicion 🔄
- Involve the multidisciplinary Endocarditis Team early for complex cases 👥
These 2023 criteria (endorsed in recent guidelines and validated through 2026) dramatically improve diagnostic accuracy - especially in tough cases - saving lives in this high-mortality disease 🫀💪
📚 Exam Tips:
👉 3 sets of blood cultures before antibiotics is the classic first step.
👉 TOE is better than TTE for prosthetic valves, abscesses, and small vegetations.
👉 Janeway lesions are painless; Osler nodes are painful.
👉 A new AV block in IE should make you think of an aortic root or peri-annular abscess.
👉 “Definite IE” in exams is often tested as 2 major or 1 major + 3 minor or 5 minor.
🧪 Investigations
- Bloods: normocytic anaemia, raised ESR/CRP
- Urine: microscopic haematuria (GN)
- ECG: arrhythmia, AV block (aortic root abscess)
- CXR: pulmonary oedema, septic emboli
- CT/MRI brain: embolic infarcts (often haemorrhagic if anticoagulated)
💊 Medical Management
- Source control: treat dental/skin sepsis
- Culture-guided IV antibiotics (see table below)
- Duration: 4–6 weeks (≥6 weeks if prosthetic valve)
- Prosthetic valve IE: triple therapy (vancomycin + gentamicin + rifampicin)
- Close liaison with Endocarditis MDT
📊 Endocarditis – Antibiotic Management Summary
| Causative Group | Recommended Treatment | Duration | Notes |
|---|---|---|---|
| Streptococcus (penicillin-sensitive) | Benzylpenicillin IV + Gentamicin (first 2 weeks) | 4 weeks | Native valve; good prognosis |
| Enterococcus | Amoxicillin IV + Gentamicin
(If penicillin allergy → Vancomycin + Gentamicin) |
4–6 weeks | High-level gentamicin resistance increasingly common |
| MSSA | Flucloxacillin IV | 4–6 weeks | ± Gentamicin first 2 weeks; avoid in renal impairment |
| MRSA / Penicillin Allergy | Vancomycin (level-adjusted) + Rifampicin ± Gentamicin | 6 weeks | Close drug-level monitoring essential |
| Prosthetic Valve Endocarditis | Vancomycin + Rifampicin + Gentamicin | ≥ 6 weeks | High mortality – always involve cardiothoracic surgery early |
| HACEK group | Ceftriaxone IV | 4 wks (native)
6 wks (prosthetic) |
Slow-growing Gram negatives |
| Fungal | Amphotericin B or Echinocandin | Prolonged | Surgery almost always required |
💡 Exam Tip: Always take 3 sets of blood cultures before starting antibiotics (unless the patient is critically unwell). ESC 2023 guidance states that at least three blood culture sets should be obtained at 30-minute intervals before antibiotics, using peripheral venepuncture and careful sterile technique. Some UK local antimicrobial guidance adds a useful practical distinction: if clinically stable, take at least three sets before antibiotics, preferably more spaced out when feasible; if septic, take three sets at 30-minute intervals so antibiotics are not delayed. Surgical referral is urgent if there is heart failure, peri-valvular abscess, uncontrolled sepsis, or large vegetations. Full antibiotic regimens must follow local protocols / latest ESC tables.
🪡 Surgical Management
- Indications: refractory infection, emboli despite therapy, HF from valve destruction, abscess
- Procedures: valve replacement (mechanical, bioprosthetic, homograft), repair where feasible, abscess drainage, device removal
- Timing: urgent if severe HF/emboli; elective if stabilised after antibiotics
Clinical signs or Stigmata of Endocarditis
Vegetations
Roth's spots

Vegetations
📚 Reference
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery