
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Migraine✅
Related Subjects:Migraine |Basilar Migraine |Cluster Headaches |Sumatriptan |Tension Headache |Analgesic Overuse Headache |Headaches in General |CADASIL
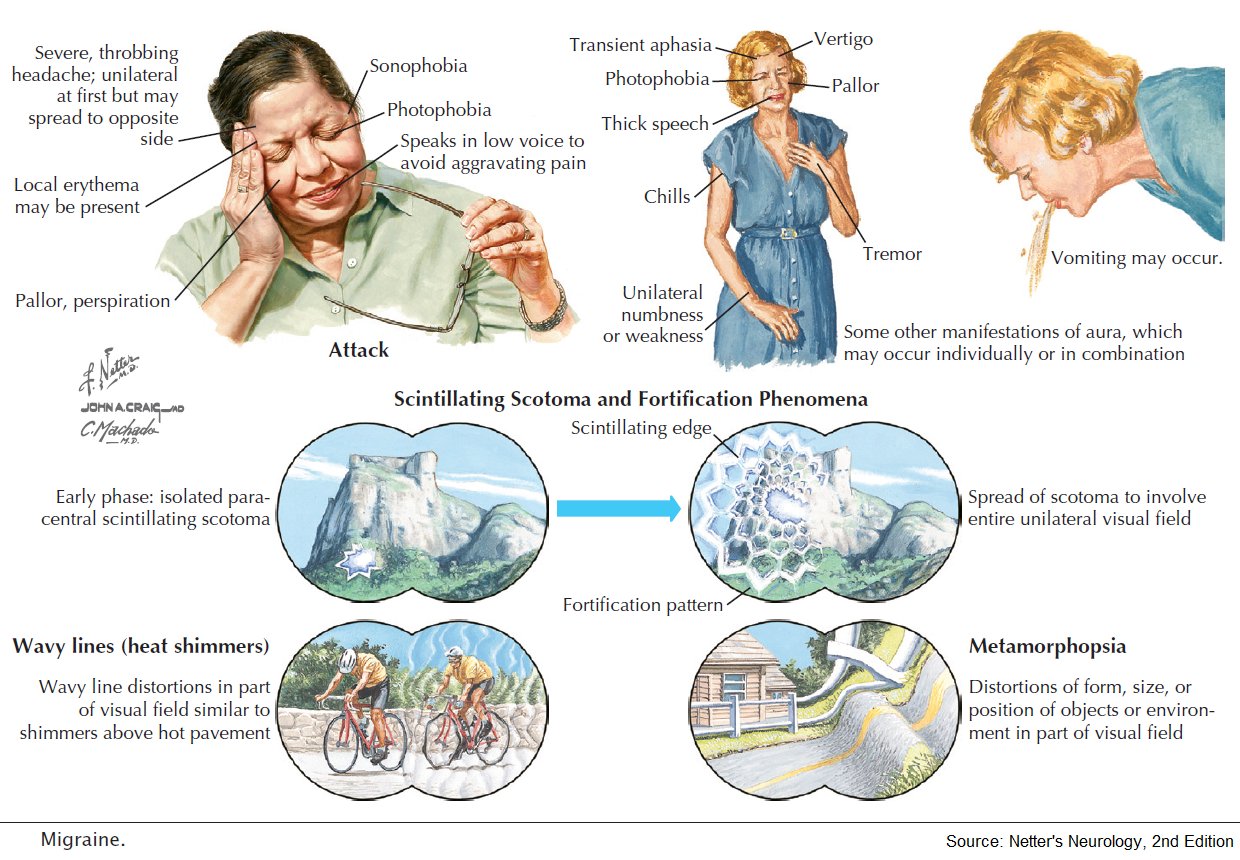
🧠 Migraine is a chronic, episodic neurological disorder causing recurrent headaches with associated features such as nausea 🤢, vomiting, photophobia 😎, and phonophobia 🔊. It affects ~1 in 10 people, more common in women (14%) than men (4%). Onset is often in childhood or young adulthood.
ℹ️ About
- ⏳ Two main types:
- Migraine without aura (common migraine)
- Migraine with aura (classical migraine)
- 🔬 Classification follows the International Classification of Headache Disorders (ICHD-2).
- 👩⚕️ Migraine is more disabling from its cognitive and sensory symptoms than from headache pain alone.
Diagnostic Criteria – Migraine without Aura
- 🔄 At least 5 attacks lasting 4–72 hours.
- ➡️ Headache has ≥2 of:
- Unilateral location 🎯
- Pulsating quality 💓
- Moderate/severe pain intensity
- Aggravated by routine activity 🏃
- During headache, ≥1 of:
- Nausea and/or vomiting 🤮
- Photophobia 😵💫 and phonophobia 📢
Diagnostic Criteria – Migraine with Aura
- ⚡ At least 2 attacks with reversible neurological symptoms:
- Visual (flickering lights ✨, scotoma 👁️)
- Sensory (pins and needles 🤲, numbness)
- Speech disturbance 🗣️
- Symptoms evolve over ≥5 minutes, last 5–60 min ⏱️, and are followed by headache within 1 hour.
🧬 Aetiology
- 🧬 Involves serotonin and CGRP dysregulation.
- 🌊 Cortical Spreading Depression (CSD): self-propagating depolarization wave → aura.
- 💓 Possible association with right-to-left shunts (e.g., PFO).
Associations
- 🧠 CADASIL (hereditary stroke disorder)
- 💔 PFO (patent foramen ovale) – controversial role in migraine with aura
- ⚡ Mitochondrial disease (MELAS)
- 🩸 Antiphospholipid antibodies & stroke syndromes
🩺 Clinical Features
- ⏱️ Duration: 4–72 hours
- 🧩 Aura in ~30% (visual, sensory, speech)
- 🤢 GI features: nausea, vomiting, diarrhoea, colic
- 🌓 Unilateral headache in ~60%, bilateral in the rest
- 🔥 Triggers: stress, let-down after stress (weekends), alcohol 🍷, cheese 🧀, lack of sleep, dehydration, exercise
🔎 Investigations
- 🧪 Usually clinical diagnosis – no tests needed in typical cases.
- ⚠️ Exclude SAH with CT ± LP if acute/atypical presentation.
- 📉 ESR for suspected temporal arteritis.
- 🫀 Bubble echo if aura + suspicion of PFO.
Migraine Variants
- 🌀 Vertebrobasilar: Diplopia, vertigo, dysarthria, stupor/coma.
- 👁️ Ophthalmoplegic: III nerve palsy, must exclude PCA aneurysm.
- 👓 Retinal: Transient monocular visual constriction.
- 🎡 Benign recurrent vertigo: Vertigo responsive to migraine therapy.
- 🩸 Menstrual migraine: Linked to hormonal changes.
These questions are used to determine your score, which then is matched to a level of disability.
- How many days in the last 3 months did you miss work or school because of your headaches?
- How many days in the last 3 months was your productivity at work or school reduced by half or more because of your headaches? (Do not include days you counted in question 1 where you missed work or school.)
- On how many days in the last 3 months did you not do household work because of your headaches?
- How many days in the last three months was your productivity in household work reduced by half or more because of your headaches? (Do not include days you counted in question 3 where you did not do household work.)
- How many days in the last 3 months did you miss family, social or leisure activities because of your headaches?
Once you have answered these questions, add up the total number of days to determine your level of disability.
| Score | Grade | Disability |
|---|---|---|
| 0 to 5 | MIDAS Grade I | Little or no disability |
| 6 to 10 | MIDAS Grade II | Mild disability |
| 11 to 20 | MIDAS Grade III | Moderate disability |
| 21+ | MIDAS Grade IV | Severe disability |
What your Physician will need to know about your headache:
- A. On how many days in the last 3 months did you have a headache? (If a headache lasted more than 1 day, count each day.)
- B. On a scale of 0 - 10, on average how painful were these headaches? (where 0 = no pain at all and 10 = pain as bad as it can be.)
⚡ Acute Migraine Management
🧠 Core idea: treat early, use adequate doses, avoid opioids, and assess for medication-overuse headache if acute treatments are being used frequently.
| Treatment | Usual adult dose / use | Key cautions |
|---|---|---|
| 🛏️ Rest / environment | Dark, quiet room; sleep can abort an attack. | Useful supportive measure but should not delay analgesia if severe. |
| 💊 NSAID
Ibuprofen |
400 mg PO, up to 600 mg if appropriate. | Avoid/caution in peptic ulcer disease, CKD, anticoagulation, severe heart failure, uncontrolled hypertension, late pregnancy. |
| 💊 NSAID
Naproxen |
500 mg PO initially, then 250 mg if needed depending on local guidance. | Longer acting; useful if recurrence occurs. Same NSAID cautions. |
| 💊 Aspirin | 900 mg PO for acute migraine. | Avoid in children <16 years, aspirin allergy, active peptic ulcer disease, significant bleeding risk, and late pregnancy unless specialist-advised. |
| 💊 Paracetamol | 1 g PO | Useful if NSAIDs contraindicated; avoid overdose and caution in severe liver disease. |
| 💊 Triptan
Sumatriptan |
50–100 mg PO, or 20 mg intranasal, or 6 mg SC for severe/rapid-onset attacks or vomiting. | Avoid in ischaemic heart disease, previous stroke/TIA, peripheral vascular disease, uncontrolled hypertension. Avoid in hemiplegic, basilar/brainstem or retinal migraine unless specialist-advised. |
| 🤢 Antiemetic
Metoclopramide / prochlorperazine |
Use for nausea/vomiting and to improve gastric emptying/absorption. Can be used even if nausea is absent. | Metoclopramide: extrapyramidal side effects, dystonia, avoid prolonged use. Prochlorperazine: sedation, dystonia, hypotension. |
| 🧬 Rimegepant | Specialist / NICE option for acute treatment in selected adults when triptans are contraindicated, not tolerated or ineffective. | CGRP receptor antagonist. Check local formulary and drug interactions. |
🧠 NICE Acute Treatment Pearls
- Offer combination treatment with an oral triptan plus an NSAID, or an oral triptan plus paracetamol.
- Consider an antiemetic even if the patient does not feel nauseated, because gastric stasis can reduce absorption during migraine.
- If one triptan fails, try another triptan or another route before concluding triptans do not work.
- Use nasal or subcutaneous triptan if vomiting, severe nausea or rapid escalation prevents oral treatment.
- Avoid opioids for migraine.
- Watch for medication-overuse headache: triptans/opioids/combination analgesics on ≥10 days/month, or paracetamol/NSAIDs on ≥15 days/month.
🛡️ Migraine Prevention — When to Consider
- Frequent, severe or disabling migraine despite good acute treatment.
- Acute medication is needed too often or medication-overuse headache is developing.
- Attacks cause significant absence from work/school or impaired quality of life.
- Contraindication, intolerance or poor response to acute treatments.
- Discuss benefits, side effects, pregnancy plans, comorbidities and patient preference before starting.
🛡️ Preventive Treatment Options
| Drug / treatment | Typical use | Important adverse effects / cautions |
|---|---|---|
| 🫀 Propranolol | Common first-line preventive option. Start low and titrate, e.g. 40 mg twice daily, adjusted to response/tolerability. | Avoid/caution in asthma, COPD with bronchospasm, bradycardia, heart block, hypotension. May cause fatigue, vivid dreams, depression, erectile dysfunction. |
| 🫀 Atenolol | Alternative beta-blocker, often off-label for migraine prevention. | Same beta-blocker cautions; dose adjust in renal impairment. |
| 🌙 Amitriptyline | Useful if insomnia, depression, anxiety, neuropathic pain or tension-type headache overlap. Start low, e.g. 10 mg nocte, titrate slowly. | Sedation, dry mouth, constipation, urinary retention, QT risk, falls risk in older adults. |
| 💊 Topiramate | Effective preventive option; start low and titrate slowly. | Paraesthesia, cognitive slowing, weight loss, mood effects, renal stones, glaucoma risk. Teratogenic; subject to UK pregnancy-prevention restrictions and avoid in pregnancy unless strict criteria met. |
| 🧃 Candesartan | Effective off-label option, especially if hypertension coexists. | Dizziness, hypotension, hyperkalaemia, renal impairment. Avoid in pregnancy. |
| 🩸 Menstrual migraine short-term prevention
Frovatriptan |
2.5 mg twice daily, usually from 2 days before expected menstruation for 5–6 days. | Useful for predictable menstrual migraine. Apply usual triptan cardiovascular cautions. |
| 💉 Botulinum toxin type A | Specialist option for chronic migraine: headache on ≥15 days/month, with migraine features on ≥8 days/month, after failure of several preventives. | Neck pain, injection-site pain, weakness, ptosis. Not used for episodic migraine. |
| 🧬 CGRP monoclonal antibodies
erenumab, fremanezumab, galcanezumab, eptinezumab |
Specialist options for frequent episodic or chronic migraine after failure of multiple preventives, depending on NICE/local criteria. | Injection/infusion reactions, constipation especially erenumab, hypersensitivity. Long-term safety and pregnancy data limited. |
| 🧬 Gepants for prevention
rimegepant / atogepant |
NICE-supported specialist options for selected adults after failure of multiple preventives. Atogepant can be used for episodic or chronic migraine prevention under NICE criteria. | Nausea, constipation, fatigue; check hepatic impairment and drug interactions. |
🚩 Red Flags — Do Not Assume Simple Migraine
- Thunderclap headache or maximal intensity at onset.
- New headache with fever, meningism, rash or reduced consciousness.
- New neurological deficit that persists or does not fit usual aura.
- New headache after age 50, cancer, immunosuppression or pregnancy/postpartum.
- Headache triggered by cough, exertion or sex.
- Progressive worsening pattern or papilloedema.
📌 Clinical Pearls
- Acute treatment works best when taken early, while pain is still mild or moderate.
- Triptans are for migraine pain, not for non-specific daily headache.
- Preventives usually need 6–8 weeks at a tolerated therapeutic dose before judging benefit.
- A useful response is often defined as around 50% reduction in migraine frequency or severity.
- Review contraception and pregnancy plans before prescribing topiramate, candesartan or newer specialist therapies.
References
Cases - Migraine
- Case 1 - Migraine Without Aura (“Common Migraine”) 💥: A 28-year-old woman presents with unilateral, throbbing headaches lasting 12 hours, associated with photophobia, phonophobia, and nausea. Attacks occur around menstruation. Diagnosis: Migraine without aura. Management: Acute: NSAID + triptan; Preventive: consider propranolol if frequent; menstrual migraine may benefit from perimenstrual triptan or hormonal therapy.
- Case 2 - Migraine With Aura (“Classic Migraine”) 🌈: A 35-year-old man reports visual zig-zag lines (scintillating scotoma) followed by unilateral headache with nausea and photophobia. Aura lasts 20 minutes and resolves before headache onset. Diagnosis: Migraine with aura. Management: Avoid vasoconstrictors if vascular risk factors; triptans for acute therapy; topiramate for prevention if frequent.
- Case 3 - Hemiplegic Migraine 🧠: A 19-year-old woman develops transient right arm weakness and dysphasia for 30 minutes, followed by severe left-sided headache. Brain imaging normal. Family history of similar attacks. Diagnosis: Familial hemiplegic migraine. Management: Avoid triptans/ergots; preventive therapy with verapamil or acetazolamide; genetic counselling.
- Case 4 - Status Migrainosus ⏳: A 40-year-old woman presents with continuous severe unilateral headache lasting >72 hours, unresponsive to her usual triptan. She has vomiting and photophobia. Diagnosis: Status migrainosus. Management: Hospital admission; IV fluids, antiemetics, IV NSAID or dihydroergotamine; exclude secondary causes.
- Case 5 - Chronic Migraine (Medication Overuse Headache) 💊: A 45-year-old man with longstanding migraine now has daily headaches. He takes OTC analgesics most days. Headaches are less severe but constant. Diagnosis: Chronic migraine with medication overuse headache. Management: Withdraw overused analgesics; introduce preventive therapy (e.g., topiramate, propranolol, botulinum toxin A if refractory); lifestyle measures.
Teaching Commentary 🧠
Migraine is a neurovascular disorder characterised by recurrent disabling headaches, often with aura. Key subtypes: - Without aura (commonest, unilateral throbbing, N/V, photophobia). - With aura (transient neurological symptoms, often visual). - Hemiplegic migraine (motor aura, mimics stroke). - Status migrainosus (prolonged, severe, emergency). - Chronic migraine (≥15 headache days/month, often with medication overuse). Management is stepwise: trigger avoidance → acute therapy (NSAIDs, triptans, antiemetics) → preventive therapy if frequent/severe (beta-blockers, topiramate, valproate, CGRP mAbs). Always consider red flags (first or worst headache, neuro deficits, papilloedema).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery