Le Fort Fractures
🦴 Le Fort I: A floating palate (horizontal).
🦴 Le Fort II: A floating maxilla (pyramidal).
🦴 Le Fort III: A floating face (transverse).
👉 Mnemonic: “Speak no evil” (I), “See no evil” (II), “Hear no evil” (III).
📖 About Le Fort Fractures
- Le Fort fractures are classical midface fractures caused by blunt trauma.
- They disrupt the structural pillars of the face → instability, malocclusion, airway risk.
- Common causes: road traffic accidents 🚗, assaults 👊, and falls 🤕.
- Airway protection and haemorrhage control are the first priorities in management.
📜 Historical Background
- Described by René Le Fort, a French surgeon, in 1901.
- He dropped cannonballs onto cadaver skulls (!) to study fracture propagation patterns.
- He boiled off soft tissues to clearly observe fracture lines - showing remarkable consistency.
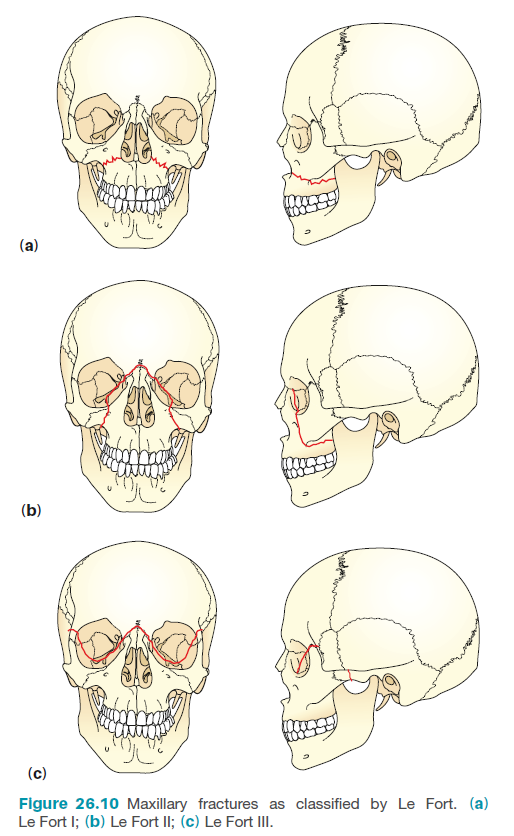
🦷 Le Fort Fractures of the Maxilla
- Le Fort I – “Floating Palate”
- Horizontal fracture above the teeth → separates hard palate from maxilla.
- Mobility of the upper dental arch when pulled.
- Often low-velocity trauma (falls, punches).
- Le Fort II – “Floating Maxilla”
- Pyramidal fracture → involves maxilla, nasal bridge, lacrimal bones, orbital floors/rims.
- Midface (nose + upper jaw) moves as a unit.
- Caused by higher-velocity impacts.
- Le Fort III – “Floating Face”
- Transverse fracture → includes nasal bridge, orbital walls, zygomatic arches.
- True craniofacial disjunction - face separates from skull base.
- Often associated with CSF leak 💧 and severe trauma.
👁️🗨️ Clinical Presentation
- Follow ATLS principles: Airway, Breathing, Circulation, Disability, Exposure.
- Signs: midface mobility, malocclusion, epistaxis, rhinorrhoea, facial bruising, periorbital swelling.
- Look for Battle’s sign, CSF leak, loose teeth, periorbital ecchymosis (“panda eyes”).
- Check GCS and pupils – associated head injury is common.
🧪 Investigations
- CT Facial Bones – gold standard for fracture definition.
- Plain films are obsolete in modern trauma practice.
- Consider CT head/c-spine if high-velocity injury.
🩺 Management of Le Fort Fractures
- Airway first 🚨
- Airway obstruction is the leading cause of death in facial trauma.
- Avoid nasotracheal intubation if skull base fracture suspected (risk of intracranial intubation).
- Consider surgical airway (tracheostomy) if needed.
- Bleeding: pack nasal/oral cavities; correct shock early.
- Secondary survey: check mobility by gently pulling on incisors.
- Give IV antibiotics (prophylaxis) and tetanus cover if indicated.
- If CSF leak present → neurosurgical referral.
- Definitive treatment: Open Reduction and Internal Fixation (ORIF) in ~60%.
30% conservative, 10% no treatment required.
📚 References
