Related Subjects:
|Classical Ventricular Tachycardia
|Idiopathic Ventricular Tachycardia
|Ventricular Fibrillation
|Resuscitation - Adult Tachycardia Algorithm
|Resuscitation - Advanced Life Support
|Atrial Flutter
|Atrial Fibrillation
|Wolff-Parkinson White syndrome (WPW)
|Supraventricular Tachycardia (SVT)
⚡ Key rule: Any regular broad-complex tachycardia should be treated as VT until proven otherwise.
If the patient is unstable, act first (shock) and diagnose later.
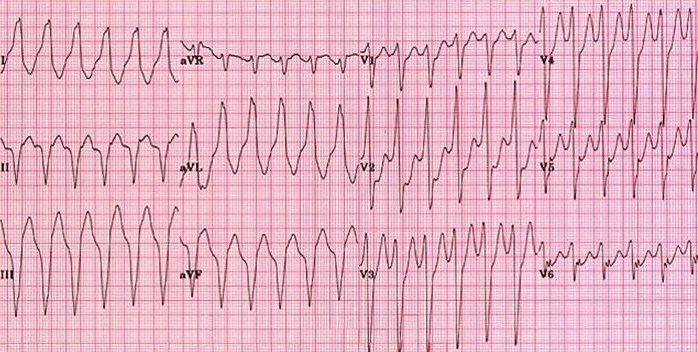
📖 Broad-Complex Tachycardia (BCT)
- Broad QRS = QRS duration >120 ms (>3 small squares).
- BCT = tachycardia with broad QRS complexes. The big fork in the road is regular vs irregular.
- Why it matters: VT can rapidly deteriorate into VF/cardiac arrest, so early, safe decision-making is crucial.
📊 Causes of BCT (regular vs irregular)
| Pattern |
Likely causes |
High-risk “don’t miss” |
| Regular BCT |
- Monomorphic VT (commonest)
- SVT with aberrancy (pre-existing BBB or rate-related BBB)
- Atrial flutter with fixed conduction + aberrancy
- Antidromic AVRT (WPW) (rare)
|
- VT (assume VT until proven otherwise)
|
| Irregular BCT |
- AF with aberrancy
- Pre-excited AF (WPW)
- Polymorphic VT / torsades de pointes
|
- Pre-excited AF (WPW) (can degenerate into VF)
- Torsades (QT-related, can deteriorate)
|
🩺 First 30 seconds: assess stability
- Unstable features: shock, syncope, ongoing chest pain/MI features, acute heart failure/pulmonary oedema, severe hypotension.
- If unstable with a pulse: synchronised DC cardioversion (sedate if conscious and time allows).
- If pulseless VT/VF: follow ALS cardiac arrest (defibrillation + CPR).
🔎 ECG clues that favour VT
| ECG/clinical clue |
Why it points to VT |
What you do with it |
| AV dissociation (P waves “march through” independently) |
Atria and ventricles are being driven by different pacemakers |
Treat as VT; urgent senior/cardiology input |
| Capture beats (a single narrow QRS during BCT) |
Occasional supraventricular impulse conducts to ventricle amid VT |
Strong VT support |
| Fusion beats (hybrid QRS morphology) |
Simultaneous ventricular activation from sinus + ventricular focus |
Strong VT support |
| Known structural heart disease / prior MI |
Scar-related re-entry VT is common in this group |
Lower your threshold to shock / treat as VT |
🧪 Investigations (don’t delay treatment if unstable)
- 12-lead ECG (if stable) + continuous monitoring.
- Bloods: U&E, Mg, Ca, glucose, FBC, troponin (if ACS possible) ± ABG/VBG if unwell.
- Echo later to assess LV function/structural disease (especially if VT suspected).
⚕️ Management table (Resus Council UK–aligned approach)
| Scenario |
Immediate action |
Key “don’ts” |
| Unstable BCT with a pulse |
- Synchronised DC cardioversion (urgent)
- Correct reversible causes (K/Mg/ischaemia, drug toxicity)
|
- Don’t “watch and wait”
- Don’t delay cardioversion for prolonged diagnostics
|
| Stable regular BCT |
- Treat as VT unless strong evidence otherwise
- Consider amiodarone IV 300 mg over 20–60 min, then infusion if needed (local protocol)
- Adenosine may be used diagnostically/therapeutically only in regular rhythms where SVT with aberrancy is plausible and expert support is available
|
- Do not use adenosine in irregular broad-complex tachycardia
|
| Stable irregular BCT |
- Think: AF with aberrancy vs pre-excited AF vs torsades
- Get senior/cardiology help early; treat reversible causes
|
- Avoid AV-nodal blockers if pre-excited AF suspected (risk of VF)
|
| Torsades de pointes (polymorphic VT + prolonged QT) |
- Correct causes: stop QT-prolonging drugs, correct K/Mg
- IV magnesium (commonly 2 g over ~10 min, then reassess; local policy)
- If unstable: DC cardioversion
|
- Don’t ignore QT prolongation (it’s the mechanism)
|
🧠 Rhythm snapshots (high-yield)
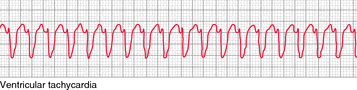
- Monomorphic VT: usually regular, broad QRS, often post-MI scar-related; can present with palpitations, syncope, or shock.
- VF / pulseless VT: cardiac arrest rhythms → ALS shockable pathway (defib + CPR).
- Pre-excited AF (WPW): irregularly irregular, very fast, varying QRS morphologies; avoid AV-nodal blockers and seek urgent expert help.
🌟 Clinical teaching point: The danger in BCT is mislabelling VT as “SVT with BBB” and giving the wrong therapy.
When myocardium is ischaemic or scarred, re-entry circuits make VT more likely; the longer it runs, the more likely it becomes haemodynamically unstable.
That’s why UK algorithms prioritise stability → shock if needed → antiarrhythmic strategy, rather than perfect rhythm diagnosis first.
📚 References (UK + core)
- Resuscitation Council UK: Tachycardia (with pulse) algorithm (peri-arrest guidance, cardioversion/antiarrhythmic approach).
- Resuscitation Council UK: Peri-arrest arrhythmias (ALS educational material).
- ESC: 2022 guidelines on ventricular arrhythmias & sudden cardiac death prevention (context for VT risk in structural heart disease).
