
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Hypothermia✅
Related Subjects: Acute Kidney Injury |Acute Rhabdomyolysis |Drowning |Hyperkalaemia |Hypothermia
❄️ “You’re not dead until you’re warm and dead.” This classic teaching point reflects the fact that severe hypothermia can profoundly suppress circulation and neurology, yet recovery may still be possible with continued resuscitation and rewarming. 💡 In accidental hypothermia, especially after rapid cooling such as cold-water immersion, survival can occur despite prolonged arrest - so do not stop resuscitation prematurely.
📘 Definition & Classification
- Hypothermia = unintentional fall in core body temperature below 35°C.
- 🌡️ Core temperature should be measured with a low-reading thermometer, ideally via a rectal, oesophageal, or other reliable core probe.
- Degrees of hypothermia:
- 🟡 Mild: 35–32°C
- 🟠 Moderate: 32–28°C
- 🔴 Severe: <28°C
- 🧭 If core temperature cannot be measured immediately, the clinical stage can be estimated from consciousness level and the presence or absence of shivering.
⚠️ Risk Factors
- 🌨️ Environmental exposure, especially prolonged cold, wind, wet clothing, immersion, or immobilisation outdoors.
- 🏚️ Homelessness, poverty, malnutrition, poor heating, and social isolation.
- 🍺 Alcohol or drug misuse, which reduce awareness, judgement, and shivering.
- 💊 Sedatives, opiates, anaesthesia, and prolonged surgery.
- 👶 Infants and young children - high surface area to volume ratio and immature thermoregulation.
- 👵 Older adults - reduced mobility, lower muscle mass, chronic illness, and poor home heating.
- 🧬 Endocrine and metabolic illness - hypothyroidism, adrenal insufficiency, hypoglycaemia.
- 🧠 Stroke, trauma, sepsis, overdose, or collapse in a cold environment.
🚨 Who is vulnerable?
Hypothermia often affects people who are cold, wet, intoxicated, immobilised, elderly, malnourished, or systemically unwell.
Always think beyond the weather - hypothermia may be a clue to an underlying medical emergency such as sepsis, myxoedema coma, adrenal crisis, or drug overdose.
🩺 Clinical Features
- 🟡 Mild hypothermia (35–32°C):
- Shivering
- Cold, pale peripheries
- Tachycardia or mild bradycardia
- Tachypnoea
- Poor coordination, slurred speech, impaired judgement
- 🟠 Moderate hypothermia (32–28°C):
- Reduced or absent shivering
- Confusion, lethargy, ataxia
- Bradycardia
- Hypoventilation
- Hyporeflexia
- Increasing risk of arrhythmia
- 🔴 Severe hypothermia (<28°C):
- Marked bradycardia and hypotension
- Coma or profound reduced consciousness
- Fixed or sluggish pupils may occur
- Atrial or ventricular arrhythmias, including VF
- Very low cardiac output or cardiac arrest
- 💥 Falls, trauma, stroke, or prolonged collapse in a cold environment may both cause and complicate hypothermia.
- 🩸 Always check blood glucose, as hypoglycaemia may mimic or worsen confusion and reduced consciousness.
🔗 Common Causes & Associations
- ❄️ Environmental exposure / immersion / avalanche / mountain or water rescue scenarios
- 🍺 Alcohol intoxication or sedative / opioid overdose
- 🏚️ Poverty, neglect, inadequate heating, homelessness
- 🧬 Myxoedema coma, adrenal insufficiency, hypoglycaemia
- 🦠 Sepsis and severe systemic illness
- 💨 Carbon monoxide poisoning
- 💥 Trauma, stroke, drowning, attempted suicide by exposure
- 🏥 Perioperative / iatrogenic hypothermia
🔎 Investigations
- 🩸 Blood tests:
- FBC - haemoconcentration or infection clues
- U&E / creatinine - dehydration, AKI
- CK - rhabdomyolysis
- Blood gas - metabolic acidosis, ventilation status, lactate
- Glucose - must be checked early
- Potassium - important prognostic marker in severe hypothermia and arrest
- TFTs if hypothyroidism suspected
- Cortisol if adrenal insufficiency is possible
- Amylase / lipase if pancreatitis suspected
- Toxicology screen where overdose or substance use is possible
- COHb if carbon monoxide exposure is suspected
- 📈 ECG:
- Sinus bradycardia
- First-degree AV block
- Prolonged PR, QRS, or QT intervals
- Atrial fibrillation
- Ventricular arrhythmias in severe cases
- Osborn (J) waves may be seen
- 🩻 Imaging:
- CT head if stroke, trauma, or intracranial pathology is suspected
- Chest X-ray if pneumonia, aspiration, pulmonary oedema, or trauma are possible
- Other imaging guided by the clinical scenario
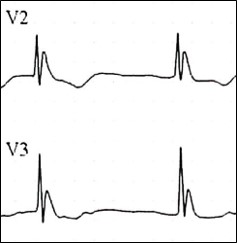
📉 ECG and Osborn (J) Waves
📈 Osborn waves are prominent positive deflections at the J point on the ECG and are classically associated with hypothermia. 💡 They become more likely as temperature falls, but they are not specific and can also occur in other conditions. Always interpret them in the context of the patient’s core temperature and clinical state.
💊 Management (Seek Senior / Critical Care Help Early)
- 🅰️ Initial stabilisation (ABCDE):
- Handle the patient gently - rough handling may precipitate ventricular fibrillation in severe hypothermia.
- Secure the airway if needed and give high-flow oxygen.
- Check breathing carefully; in severe hypothermia, respiration may be very slow.
- Check for signs of life and central pulse for up to 1 minute if profoundly hypothermic.
- Gain IV / IO access and start continuous cardiac monitoring.
- Prevent further heat loss immediately: remove wet clothing, dry the patient, insulate, and keep the environment warm.
- 🔥 Rewarming strategies:
- 🟡 Mild hypothermia (32–35°C): passive external rewarming - warm room, blankets, dry clothing, warm oral fluids if fully conscious.
- 🟠 Moderate hypothermia (<32°C): active external rewarming - forced-air warming, heated blankets, warmed IV fluids.
- 🔴 Severe hypothermia / instability / arrest: active internal rewarming may be needed - warmed humidified oxygen, warmed IV fluids, cavity lavage in selected cases, and in the most severe cases extracorporeal rewarming (ECMO / bypass).
- ❤️ Cardiac arrest in hypothermia:
- Continue resuscitation while active rewarming is underway.
- Defibrillation and drugs may be less effective at very low core temperatures, but advanced life support should not be abandoned prematurely.
- Extracorporeal life support may be lifesaving in selected patients.
- 🧪 Additional measures:
- Monitor glucose, potassium, and acid–base status closely.
- Treat hypoglycaemia promptly.
- Consider thiamine if malnourished or alcohol dependent.
- Consider naloxone if opioid overdose is possible.
- If myxoedema coma or adrenal crisis is suspected, treat urgently with appropriate endocrine support and steroids.
- 🎯 Treat the cause:
- Sepsis → antibiotics and source control
- Hypothyroidism → thyroid hormone replacement
- Adrenal insufficiency → hydrocortisone
- Overdose / poisoning → antidotes and supportive care
- Trauma / stroke → directed investigation and management
🧠 Practical Pearls
- ❄️ Not all hypothermia is “just exposure” - always look for an underlying precipitant.
- 🫀 Bradycardia in hypothermia is often physiological; do not rush to pace unless there is failure to improve with rewarming.
- 🩸 A very high potassium in hypothermic arrest is a poor prognostic sign.
- 🚑 Severe hypothermia with instability should prompt early discussion with critical care / ECMO-capable centres where available.
📚 References
- Resuscitation Council UK – Special Circumstances: Accidental Hypothermia
- StatPearls – Hypothermia
- NICE CG65 – Inadvertent Perioperative Hypothermia
📖 Cases – Hypothermia
- Case 1 – Environmental exposure ❄️: A 72-year-old homeless man is found outdoors in winter, drowsy and shivering. Core temperature 32°C. Exam: bradycardia, slurred speech, slow reflexes. ECG shows J waves. Diagnosis: moderate accidental hypothermia due to environmental exposure. Managed with insulation, warmed IV fluids, active external rewarming, and investigation for infection, hypoglycaemia, and other contributors.
- Case 2 – Iatrogenic 🏥: A 64-year-old woman undergoing prolonged abdominal surgery develops a core temperature of 34°C. She has cold peripheries, coagulopathy, and metabolic acidosis. Diagnosis: perioperative hypothermia. Managed with forced-air warming, warmed IV fluids, and active temperature monitoring.
- Case 3 – Secondary to metabolic illness 🧬: A 55-year-old man with known hypothyroidism is brought in confused and hypothermic at 30°C. He is bradycardic, hypotensive, and has dry skin. TFTs show severe hypothyroidism. Diagnosis: myxoedema coma with severe hypothermia. Managed in ICU with thyroid hormone replacement, hydrocortisone, careful rewarming, and supportive care.
🩺 Teaching Point:
Hypothermia = core temperature <35°C.
🟡 Mild: shivering, cold stress, impaired coordination
🟠 Moderate: confusion, bradycardia, reduced shivering
🔴 Severe: coma, arrhythmias, cardiac arrest
Think of causes in 2 groups: exposure and secondary medical causes.
Management = ABCDE + prevent further heat loss + rewarm appropriately + treat the trigger.
⚠️ In severe hypothermia, handle gently and do not stop resuscitation too early.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery