
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Pharynx
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
The pharynx is a fibromuscular tube that serves as the shared pathway for air, food, and liquids. It extends from the base of the skull to the upper oesophagus (approximately C6), sitting posterior to the nasal and oral cavities and superior to the larynx. Its functions are tightly integrated: swallowing (safe bolus transit), breathing (air conduction), speech resonance, and immune surveillance via Waldeyer’s ring. Clinically, pharyngeal anatomy underpins airway management, ENT infections, sleep apnoea, and head & neck cancer pathways.
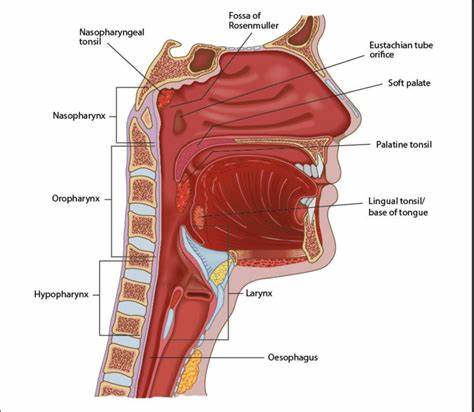
📍 Subdivisions of the Pharynx
The pharynx is divided into nasopharynx, oropharynx, and laryngopharynx (hypopharynx). Each has distinctive epithelium, landmarks, and clinical problems. A helpful framework is: nasopharynx = airway + pressure equalisation, oropharynx = airway + food pathway, laryngopharynx = decision point (air to larynx, food to oesophagus).
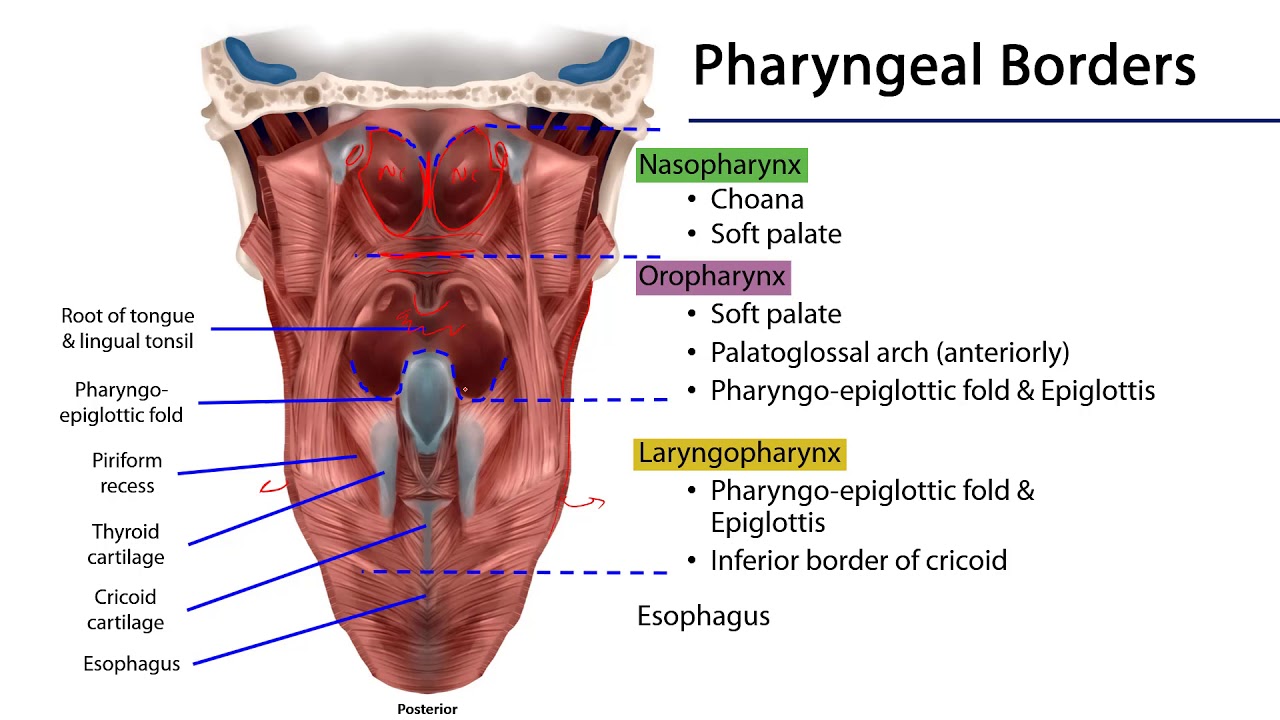
- 👃 Nasopharynx (behind nasal cavity; above soft palate)
- Boundaries: skull base (roof) → soft palate (floor).
- Connections: communicates with nasal cavity via choanae.
- Key structures:
- Pharyngeal tonsil (adenoids) in roof/posterior wall (Waldeyer’s ring).
- Opening of the pharyngotympanic (Eustachian) tube on lateral wall (torus tubarius).
- Epithelium: respiratory (ciliated pseudostratified columnar) → mucus clearance.
- Clinical: adenoidal hypertrophy → nasal obstruction, snoring, hyponasal speech, recurrent otitis media/effusions (tube dysfunction).
- 👄 Oropharynx (soft palate → upper border of epiglottis / level of hyoid)
- Key structures:
- Palatine tonsils in tonsillar fossa between anterior and posterior faucial pillars.
- Base of tongue and lingual tonsil.
- Fauces = gateway from mouth to pharynx.
- Epithelium: stratified squamous (abrasion-resistant).
- Clinical: tonsillitis, peritonsillar abscess (quinsy), referred otalgia via glossopharyngeal sensory pathways; HPV-related oropharyngeal cancer.
- Key structures:
- 🗣️ Laryngopharynx (Hypopharynx) (epiglottis/hyoid region → cricoid cartilage; continues as oesophagus)
- Functionally: directs food posteriorly into oesophagus and air anteriorly into larynx.
- Key spaces:
- Piriform fossae (recesses lateral to laryngeal inlet) - common site for foreign body lodging.
- Postcricoid region and posterior pharyngeal wall.
- Epithelium: stratified squamous.
- Clinical: hypopharyngeal cancers often present late; foreign bodies can injure mucosa; aspiration risk if coordination fails.
🧱 Wall Structure & Fascial Planes
The pharyngeal wall is layered to allow a delicate balance: a protective mucosa, a muscular “pump” for swallowing, and fascial layers that anchor the pharynx to the skull base and separate it from critical deep neck spaces. These fascial planes explain how deep neck infections can spread.
- Mucosa: epithelium varies by region:
- Nasopharynx: respiratory epithelium for mucociliary clearance.
- Oro-/laryngopharynx: stratified squamous to resist mechanical abrasion.
- Submucosa: contains minor salivary glands, lymphoid tissue (Waldeyer’s ring components), vessels, and connective tissue.
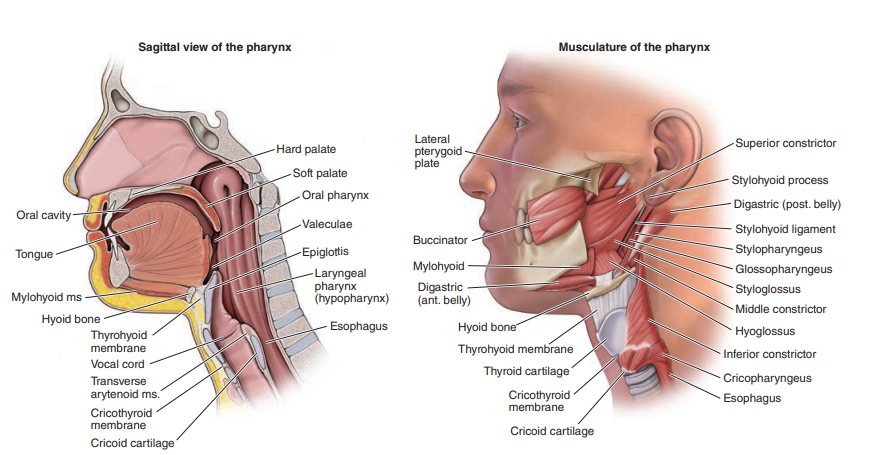
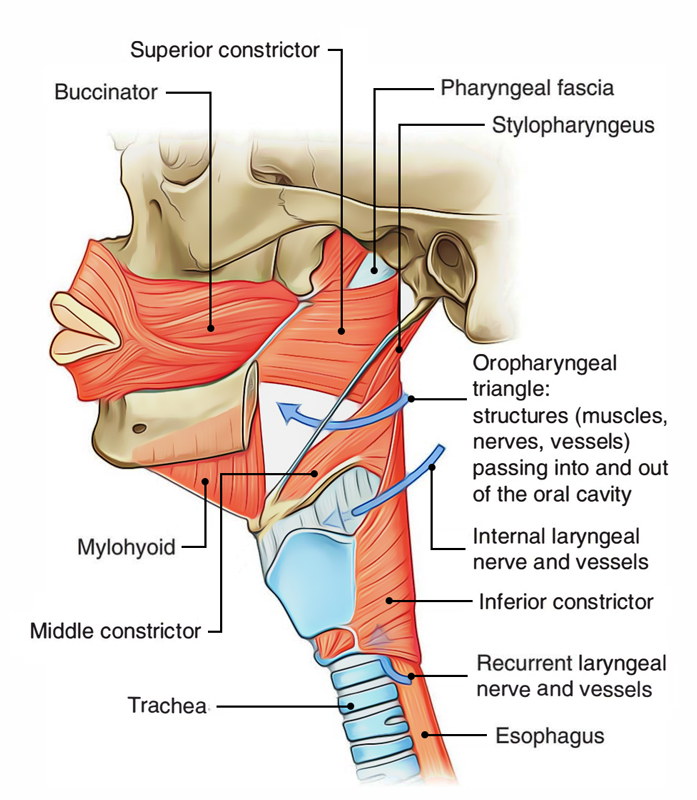
- Muscular layer:
- Outer circular constrictors propel the bolus:
- Superior constrictor
- Middle constrictor
- Inferior constrictor (includes cricopharyngeus = major part of upper oesophageal sphincter)
- Inner longitudinal muscles elevate and widen the pharynx during swallowing:
- Stylopharyngeus (key: innervated by CN IX)
- Palatopharyngeus
- Salpingopharyngeus
- Outer circular constrictors propel the bolus:
- Fascial layers:
- Pharyngobasilar fascia helps attach the pharynx to the skull base (important where muscle is thinner superiorly).
- Buccopharyngeal fascia on the outer surface; separates pharynx from the retropharyngeal space.
- Clinical: retropharyngeal infections can descend into the mediastinum (“danger space” anatomy concept).
🩸 Blood Supply, Venous Drainage & Lymphatics
- Arterial supply: predominantly branches of the external carotid artery:
- Ascending pharyngeal artery (high-yield)
- Facial, lingual, maxillary contributions
- Superior thyroid contributions (especially inferior regions)
- Venous drainage: pharyngeal venous plexus → internal jugular vein (via pharyngeal veins).
- Lymphatics:
- Nasopharynx → retropharyngeal nodes and upper deep cervical nodes.
- Oropharynx → upper deep cervical nodes (jugulodigastric prominent in tonsillitis).
- Hypopharynx → deep cervical nodes (can be bilateral depending on site).
🧠 Innervation (Sensory + Motor)
Innervation is via the pharyngeal plexus (mainly CN IX and X with sympathetic fibres). A safe exam rule: motor is mostly CN X (except stylopharyngeus = CN IX), while sensation is region-specific (V2, IX, X). This wiring explains the gag reflex and aspiration risk when sensation is impaired.
- Motor:
- CN X (vagus) via pharyngeal plexus supplies most pharyngeal muscles (constrictors + most longitudinal muscles).
- CN IX (glossopharyngeal) supplies stylopharyngeus (classic exception).
- Sensory:
- Nasopharynx: primarily CN V2 (maxillary division of trigeminal).
- Oropharynx: primarily CN IX.
- Laryngopharynx: primarily CN X (via internal laryngeal branch for laryngeal inlet region).
- Gag reflex (high yield):
- Afferent: CN IX
- Efferent: CN X
⚙️ Physiology: What the Pharynx Actually Does
🥣 1) Swallowing (Deglutition)
Swallowing is a precisely timed sequence that converts a shared aero-digestive tube into a protected food channel. The oral phase is voluntary, but the pharyngeal phase is a stereotyped reflex coordinated by the brainstem swallowing centre. Key goals: propel the bolus efficiently while preventing aspiration into the larynx and avoiding nasal regurgitation.
- Soft palate elevation seals the nasopharynx → prevents nasal regurgitation.
- Pharyngeal elevation and shortening (longitudinal muscles) creates a receptive “funnel”.
- Sequential constrictor contraction propels bolus downward.
- Laryngeal protection: larynx elevates and moves anteriorly; vocal folds close; epiglottis deflects posteriorly.
- Upper oesophageal sphincter (cricopharyngeus) relaxes to allow bolus entry into oesophagus, then re-tones to prevent air entry and reflux upward.
🌬️ 2) Respiration (Airflow Conduction)
- Pharynx provides a compliant airway segment; patency is maintained by muscle tone, especially during inspiration.
- Sleep physiology: reduced pharyngeal dilator tone predisposes to upper airway collapse → central to OSA mechanisms.
🎶 3) Speech & Resonance
- The pharynx acts as a resonating chamber that shapes sound produced by the larynx.
- Soft palate position controls nasal vs oral resonance (velopharyngeal closure).
🧬 4) Immune Function (Waldeyer’s Ring)
- Waldeyer’s ring provides immunological sampling at the entry to the GI and respiratory tracts:
- Adenoids (pharyngeal tonsil)
- Palatine tonsils
- Lingual tonsil
- Tubal tonsils
- Important for early-life pathogen defence but can hypertrophy or become chronically infected.
⚠️ Clinical Significance (High yield)
- Obstructive sleep apnoea (OSA): collapse of the oropharyngeal airway during sleep due to reduced dilator tone and anatomical crowding.
- Tonsillitis / Quinsy: peritonsillar abscess causes severe sore throat, uvular deviation, “hot potato” voice, trismus; can threaten airway.
- Nasopharyngeal carcinoma: often presents with cervical lymphadenopathy, nasal obstruction/epistaxis, conductive hearing loss (Eustachian tube dysfunction); associated with EBV.
- Zenker’s diverticulum: pulsion diverticulum above the upper oesophageal sphincter (Killian’s dehiscence) → dysphagia, regurgitation, aspiration, halitosis.
- Foreign body: can lodge in piriform fossa; consider mucosal injury and aspiration risk.
- Cranial nerve lesions: IX/X dysfunction → dysphagia, nasal regurgitation, aspiration; abnormal gag and palate asymmetry.
✅ Conclusion
The pharynx is the core of the aero-digestive tract, coordinating airflow with safe swallowing while shaping speech resonance and hosting essential lymphoid defences. Understanding the regional epithelium, muscle layers, and nerve supply (V2/IX/X) explains common ENT presentations from otitis media and OSA to quinsy and head & neck malignancy. 🔑 Exam pearl: gag reflex = afferent CN IX, efferent CN X; stylopharyngeus is the classic CN IX motor exception.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery