
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Abdomen - Perforation of a Viscus
Related Subjects:Acute Cholecystitis |Acute Appendicitis |Chronic Peritonitis |Acute Abdomen - Perforation of a Viscus |Abdominal Aortic Aneurysm |Ectopic Pregnancy |Acute Cholangitis |Acute Abdominal Pain |Penetrating Abdominal Trauma |Abdominal Masses: Clinical Approach and Considerations |Abdominal Distension |Vomiting
🩻 CT scan abdomen is the gold standard and more sensitive than plain films for suspected GI perforation. ⚠️ Findings may be masked in elderly or immunosuppressed patients.
📖 About
- Perforation of a gas- and bacteria-containing GI tract anywhere from oesophagus ➝ anus.
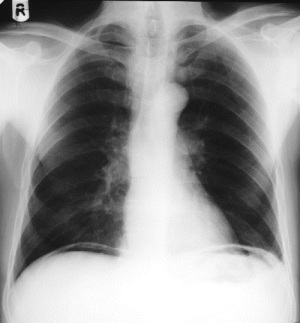
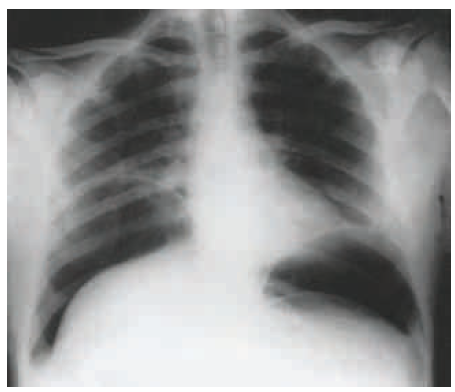
- 💨 Gas rises and can be seen trapped under the diaphragm on an erect CXR.
- Perforation leads to free intraperitoneal air and spillage of luminal contents → bacterial peritonitis + sepsis.
🧬 Aetiology
- Can occur at any point in the GI tract.
- Always consider in any patient presenting with an acute abdomen.
- Free air = red flag for overwhelming bacterial peritonitis and septic shock if untreated.
📸 Imaging: Free Air

⚠️ Causes
- Oesophagus: Caustic ingestion, endoscopic biopsy/dilatation, Boerhaave syndrome (post-vomiting), oesophageal tumour, chest trauma.
- Stomach: Peptic ulcer disease, NSAID-induced erosion, gastric cancer, penetrating trauma.
- Small bowel: Ischaemia, Crohn’s disease (fistula/erosion), trauma.
- Large bowel: Toxic megacolon (C. difficile, UC), diverticulitis, polypectomy/perforation during colonoscopy, trauma, cancer.
🩺 Clinical Features
Findings may be subtle in elderly or chronically immunosuppressed patients.
- 🚨 Sudden severe abdominal pain, worsened by movement.
- Rigidity, rebound, and percussion tenderness (“board-like abdomen”).
- Absent bowel sounds.
- Fever, tachycardia, hypotension (sepsis/shock).
- May coexist with bowel obstruction, diverticulitis, or malignancy.
🔍 Differentials
- Acute pancreatitis
- Myocardial infarction (can mimic upper abdo pain)
- Tubo-ovarian pathology (ruptured cyst, torsion)
- Ruptured abdominal aortic aneurysm (AAA)
🧪 Investigations
- 🩸 Bloods: FBC, U&E, LFTs, amylase, CRP – often raised WCC/CRP.
- 🩻 Plain films: CXR/AXR → free air under diaphragm, Rigler’s sign (air both sides of bowel wall), loss of psoas outline.
- 💧 Contrast swallow → useful if oesophageal perforation suspected.
- 🖥️ CT Abdomen = gold standard (sensitive for free air, perforation site, complications).
💉 Management
- 🚫 Nil by mouth (NPO).
- ABC resuscitation: IV fluids, oxygen, monitoring, analgesia.
- Broad-spectrum IV antibiotics (cover Gram-negatives + anaerobes).
- Immediate surgical review:
- Perforation repair or resection (laparotomy/laparoscopy).
- Selected cases (contained leak, stable patient) → conservative management with close observation.
- Consider ITU/HDU support if unstable.
📚 References
- NICE guidance on acute abdomen and GI emergencies.
- BNF – Antibiotic regimens for intra-abdominal sepsis.
- RCS guidelines on management of hollow viscus perforation.
📝 Revisions
- Updated September 2025
3 Clinical Cases - Gastrointestinal Perforation of a Viscus ⚠️🩻
- Case 1 - Perforated peptic ulcer 🥼: A 48-year-old man with a history of NSAID use presents with sudden-onset severe epigastric pain radiating to the shoulder. He lies motionless, abdomen rigid with rebound tenderness. CXR: free air under the diaphragm. Teaching: A perforated duodenal ulcer is the classic cause of acute peritonitis with “board-like” abdomen. Urgent surgical repair (e.g. Graham patch) + IV fluids, antibiotics, and NG tube decompression are indicated.
- Case 2 - Perforated diverticulitis 🌿: A 72-year-old woman with left lower quadrant pain, fever, and constipation develops worsening peritonitis and hypotension. CT abdomen: sigmoid diverticulitis with free air and fluid. Teaching: Diverticular perforation often presents in older patients and carries high mortality. Management depends on severity: IV antibiotics, percutaneous drainage if contained abscess, or emergency colectomy with stoma (Hartmann’s procedure) for free perforation.
- Case 3 - Iatrogenic perforation (colonoscopy) 💉: A 64-year-old man undergoes colonoscopy for polyp surveillance and develops acute abdominal pain and tachycardia post-procedure. AXR: large amount of free intraperitoneal air. Teaching: Colonoscopic perforation is a recognised complication. Prompt recognition is vital - management ranges from conservative (if stable, small perforation, minimal peritonitis) to urgent surgical repair. Always suspect when abdominal pain occurs after endoscopy.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery