Fractured Shaft Femur
Related Subjects:
|Fracture management basics
|Fractured Neck of Femur
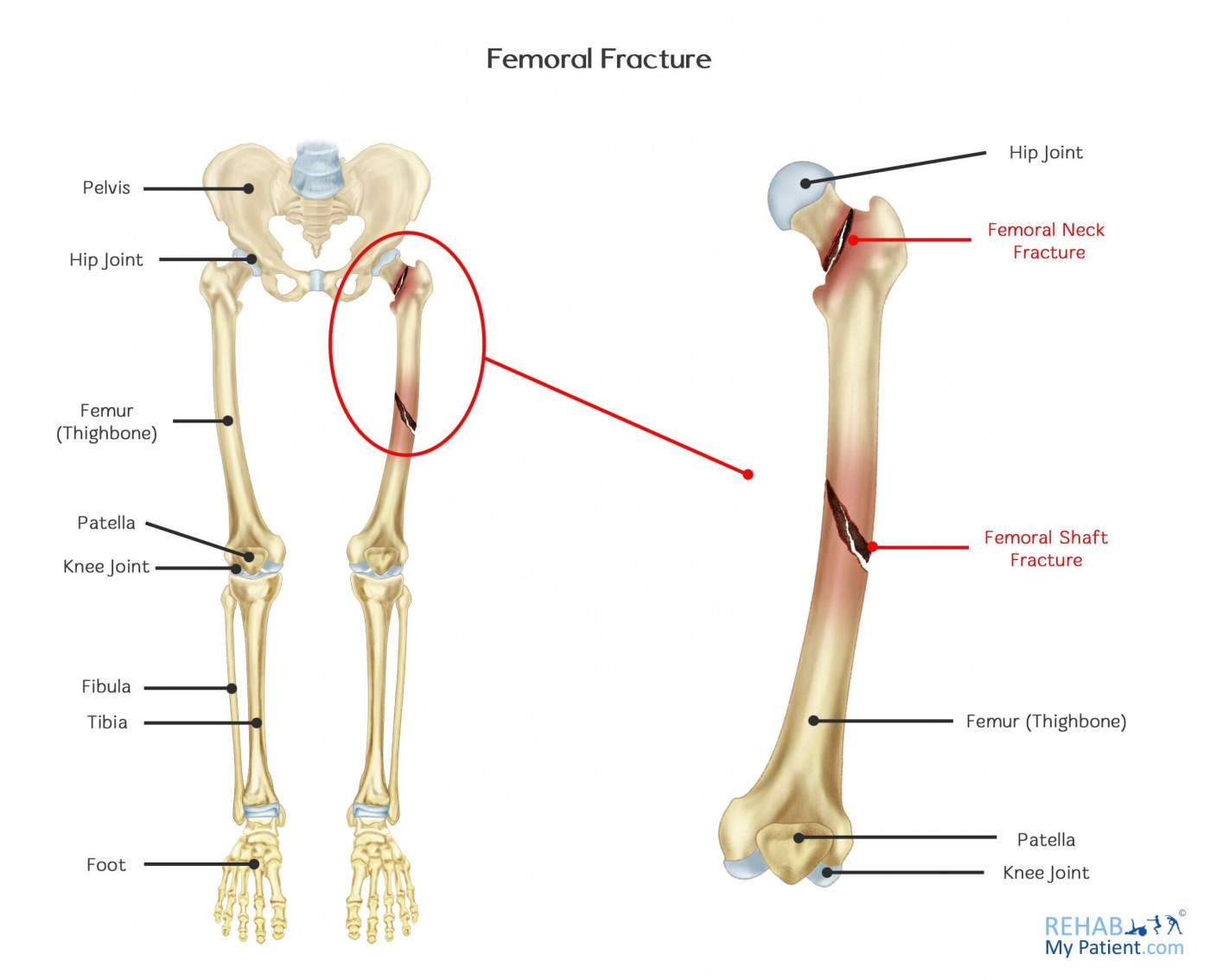
|Fractured Shaft Femur
|Fractured Femur Supracondylar Fractures
|Fractured Femur
|Fractured Tibia and Fibula
Femoral Shaft Fractures 🦴🚨 are usually caused by high-energy trauma such as road traffic collisions or falls from height, and should prompt assessment for major trauma and occult blood loss.
If the mechanism seems minor or disproportionate to the injury, always consider a pathological or insufficiency fracture caused by osteoporosis, malignancy, metabolic bone disease, Paget disease, or infection.
📖 About
- The femur is the longest and strongest bone in the body, so a shaft fracture in a healthy adult usually implies major force.
- The femoral shaft is the diaphyseal portion between the subtrochanteric region proximally and the supracondylar region distally.
- These injuries are important not only because of the bone injury itself, but because they can be associated with major haemorrhage, fat embolism, open injury, vascular compromise, and polytrauma.
⚙️ Aetiology
- High-energy trauma: road traffic collisions, falls from height, crush injury, gunshot injury.
- Low-energy/pathological fracture: osteoporosis, metastatic disease, primary bone tumour, Paget disease, osteomyelitis, or other metabolic bone disease.
- Periprosthetic fracture: may occur around existing femoral implants or hip/knee arthroplasty.
🔎 Types
- Transverse: usually from bending force.
- Oblique: diagonal fracture line.
- Spiral: torsional mechanism.
- Comminuted / segmental: suggests high-energy injury with greater soft-tissue damage.
- Open fracture 🚨: skin breach communicating with the fracture or deep tissues, with increased risk of contamination and infection.
- Pathological fracture: fracture through abnormal bone, often after trivial trauma.
🩺 Clinical Features
- Severe thigh pain and inability to weight-bear.
- Visible deformity, swelling, shortening, and often external rotation of the limb.
- Thigh swelling may be marked because the femur can bleed significantly into the surrounding soft tissues.
- Open wounds, skin tenting, or bruising may indicate severe soft-tissue injury.
- Always assess for other injuries, especially pelvic, hip, knee, chest, abdominal, head, and vascular trauma in high-energy mechanisms.
🚨 Immediate Dangers / Complications
- Haemorrhage and shock: a femoral shaft fracture can conceal major blood loss into the thigh.
- Open fracture: infection risk and soft-tissue loss.
- Neurovascular compromise: distal ischaemia, evolving nerve deficit, absent or reduced pulses.
- Compartment syndrome: pain out of proportion and pain on passive stretch are early warning signs.
- Fat embolism syndrome: classically develops 24–72 hours later with hypoxia, confusion, and petechiae.
- VTE: DVT and PE risk is increased after major lower-limb trauma.
- Delayed union, non-union, malunion, infection, especially in open or highly comminuted injuries.
🧪 Investigations
- X-rays: AP and lateral imaging of the entire femur, including the hip and knee joints.
- CT: if there is concern about extension into the hip or knee, complex fracture morphology, associated pelvic injury, or major trauma.
- Bloods: FBC, U&Es, coagulation profile, lactate, and group and save / crossmatch in significant trauma.
- Trauma imaging: in a polytrauma patient, imaging should be integrated into the broader trauma pathway rather than treating the femur injury in isolation.
💊 Initial Management
- Follow ABCDE first and treat as major trauma where appropriate.
- Give early analgesia and reassess regularly.
- Document distal pulses, capillary refill, motor function, and sensation before and after splintage or reduction.
- In the pre-hospital setting, NICE recommends considering a traction splint or the adjacent leg as a splint for suspected long-bone fractures above the knee.
- Immobilise the limb promptly to reduce pain, bleeding, and further soft-tissue injury.
- In a shocked patient, resuscitate appropriately and look for associated bleeding sources; do not assume the femur is the only explanation.
🩹 Open Femoral Shaft Fracture
- Assume any wound near the fracture is an open fracture until proven otherwise.
- Do not irrigate open long-bone fractures in the emergency department before formal wound excision.
- Cover with a saline-soaked dressing and an occlusive layer.
- Give IV prophylactic antibiotics immediately if not already given.
- Check tetanus status according to local policy.
- Realign and splint the limb, and involve orthopaedics urgently.
- Open long-bone fractures should be managed using an orthoplastic approach, with timing of wound excision based on contamination and injury severity.
🔧 Definitive Management
- Most adult femoral shaft fractures require operative fixation.
- Intramedullary nailing is the usual definitive treatment for most adult diaphyseal femoral shaft fractures because it provides strong load-sharing fixation and allows earlier mobilisation.
- Plate fixation may be used in selected fractures, especially where the fracture extends proximally or distally, where nailing is not feasible, or in some periprosthetic patterns.
- External fixation may be used temporarily in unstable polytrauma as part of damage control orthopaedics.
- Pathological fractures often need a more individualised plan, including investigation of the underlying lesion and sometimes biopsy before or during fixation.
🧑⚕️ Rehabilitation and Ongoing Care
- Start physiotherapy early once the patient is stabilised.
- Weight-bearing depends on fixation method, fracture pattern, and surgeon advice.
- Provide VTE prophylaxis according to hospital policy and bleeding risk; this is standard prophylaxis, not treatment of the fracture itself.
- In older adults or low-energy fractures, assess for fragility, osteoporosis, falls risk, and underlying malignancy.
📌 OSCE / Exam Pearls
- Always say: ABCDE, analgesia, splintage, neurovascular exam, whole-femur imaging, and look for associated injuries.
- A femoral shaft fracture can cause major concealed blood loss and should be treated with the same seriousness as other major trauma injuries.
- Any wound near the fracture = open fracture until proven otherwise.
- Open fracture management in UK guidance is antibiotics + saline-soaked occlusive dressing + splintage + urgent orthopaedic/orthoplastic input, not ED wound washout.
- Fat embolism is a classic delayed complication: respiratory distress + neurological change + petechial rash.
📚 References