Related Subjects:
|Medulla Oblongata
|Midbrain
|Pons
|Caudate Nucleus
|Putamen and Globus Pallidus
|Cerebral Cortex
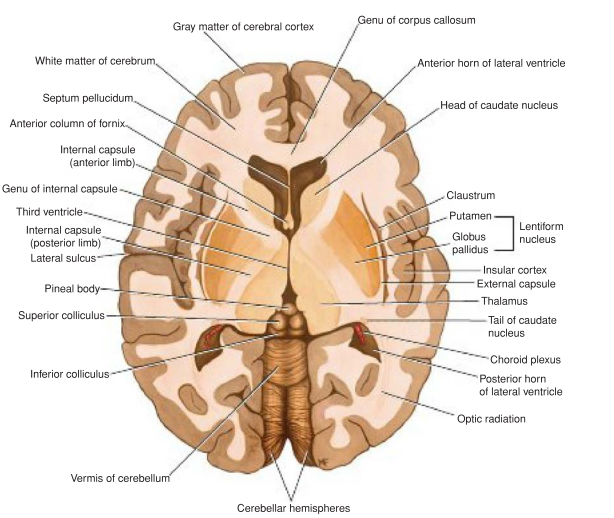
|Internal Capsule
|Cavernous sinus
|Basal Ganglia
|Medulla Oblongata
|Midbrain
|Pons
|Cavernous sinus
|Brainstem Anatomy
|Thalamic Anatomy
|Caudate Nucleus
🔬Anatomy
ℹ️ About
- The cerebral cortex is a thin grey layer of neuronal cell bodies and connections overlying the cerebrum 🌐.
- Thickness varies: Motor cortex (~4.5 mm, thickest), visual cortex (~1.5 mm, thinnest).
- Input: Mainly to Layers II & IV. Output: Mainly from Layers V & VI.
Anatomy & Histology
Cortical Layers
- Layer I: Molecular layer – few cells, mainly synaptic connections.
- Layer II: External granular layer – input from other cortical areas.
- Layer III: External pyramidal layer – output to association & commissural fibres.
- Layer IV: Internal granular layer – receives thalamocortical input (e.g. lateral geniculate → visual cortex 👁️).
- Layer V: Internal pyramidal layer – output to corticospinal, corticobulbar, striatum. Contains large Betz cells in motor cortex 💪.
- Layer VI: Multiform layer – corticothalamic output.
Cerebral Architecture
- ~5 mm of grey matter overlying white matter tracts.
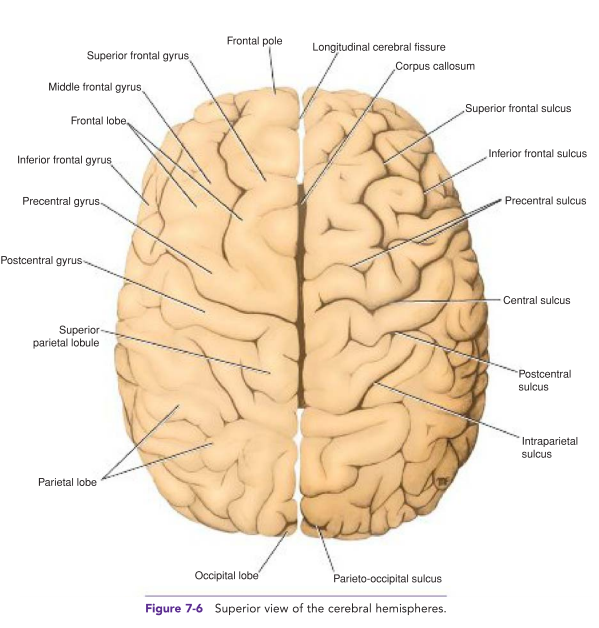
- Surface area expanded by gyri & sulci to maximise processing capacity.
- Columnar organisation: neurons arranged vertically, sharing functional roles.
- Brodmann (1909): Mapped cortex into ~52 areas by cellular micro-architecture – still clinically useful 🧩.
- Clinical note: Broca’s area discovery (expressive dysphasia from left inferior frontal lesion) provided early evidence for localisation of function.
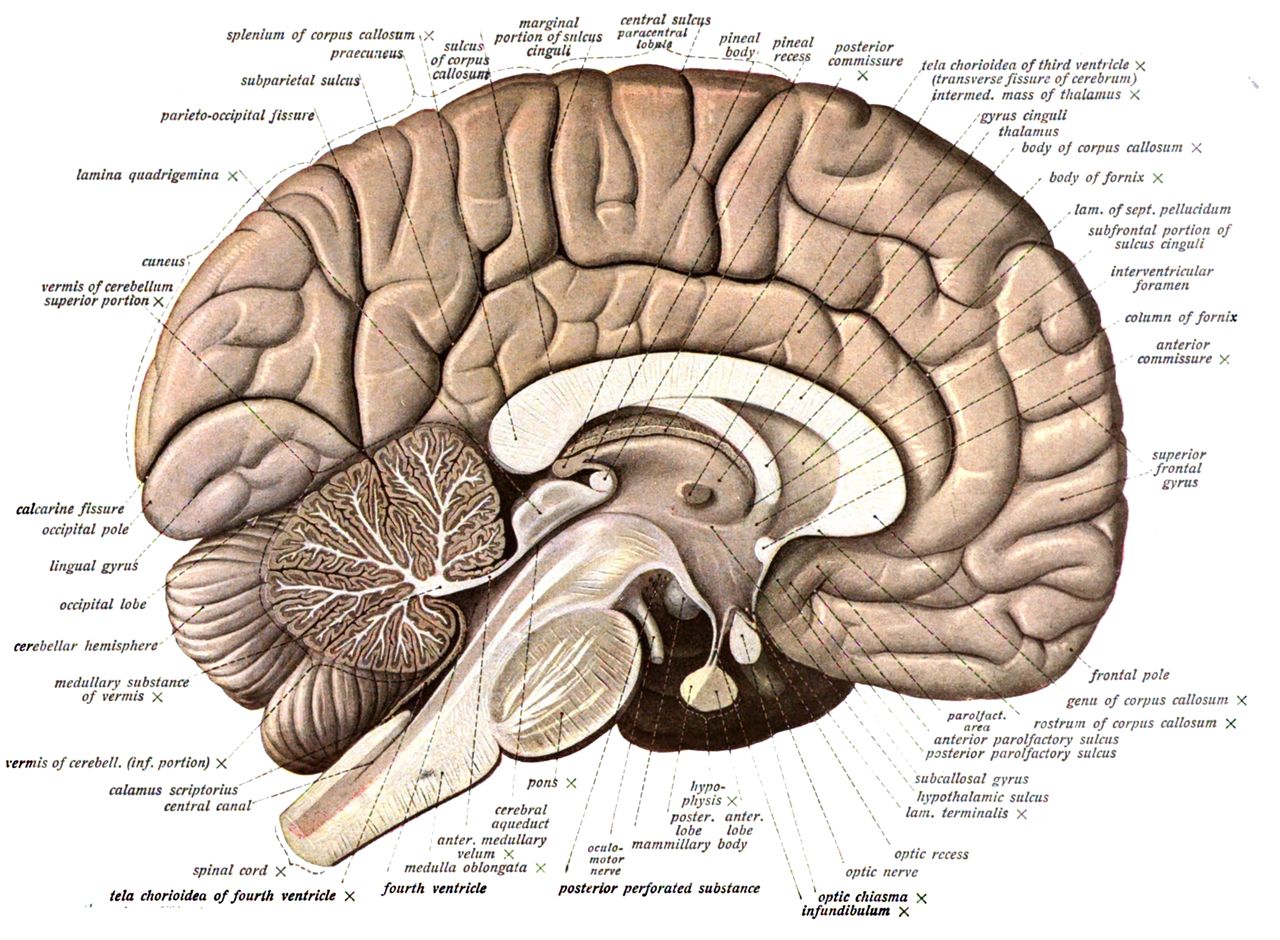
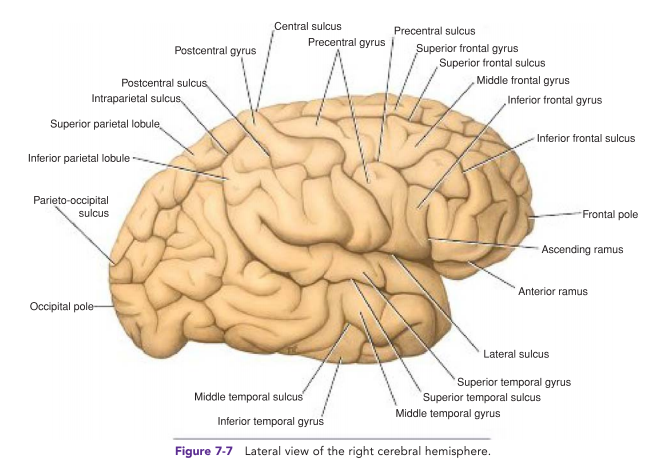
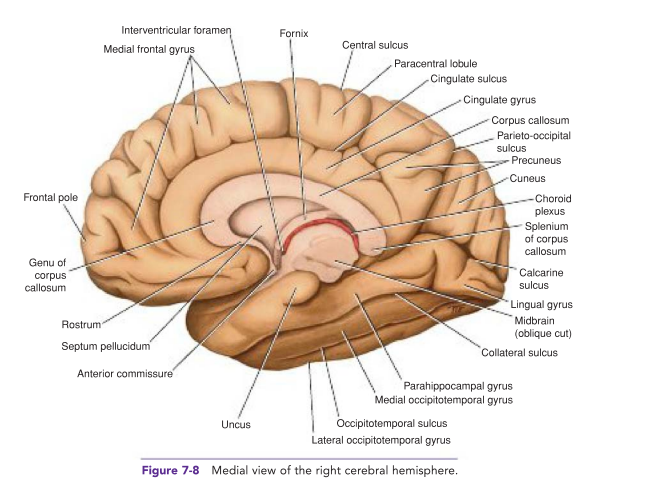
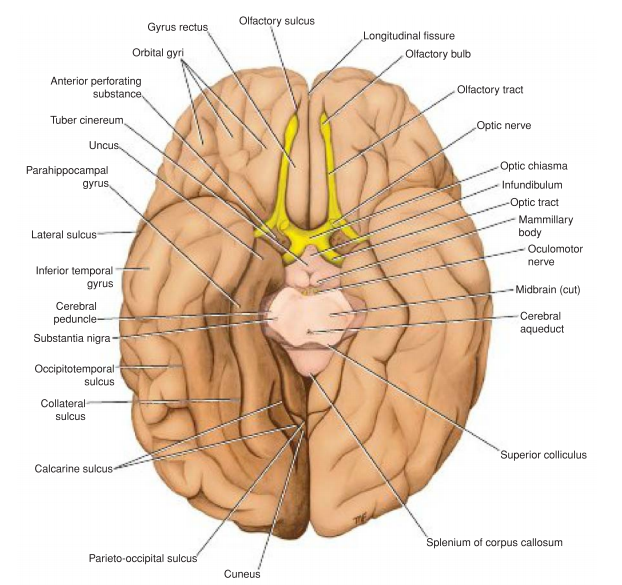
Important Sulci for Orientation
- Central sulcus: Divides frontal (motor) & parietal (sensory) cortices.
- Lateral (Sylvian) fissure: Superior border of temporal lobe.
- Parieto-occipital sulcus: Separates parietal from occipital lobe.
- Cingulate sulcus: Above corpus callosum (limbic region).
- Preoccipital notch: Border of occipital lobe.
Lobes & Functions
- Frontal lobe:
- Primary motor cortex: Voluntary movement (homunculus 🖐️👄🦵).
- Premotor & supplementary areas: Planning movement.
- Frontal eye fields: Eye movement control.
- Broca’s area (dominant side): Speech production – lesion → expressive dysphasia.
- Prefrontal cortex: Executive function, personality, judgement.
- Parietal lobe:
- Primary somatosensory cortex: Sensation mapping (hand & face laterally, leg medially).
- Association cortex: Integration of sensory input.
- Clinical: Right parietal lesions → neglect, left parietal → dyscalculia, dysgraphia.
- Temporal lobe:
- Auditory cortex: Superior temporal gyrus, input from medial geniculate body 👂.
- Wernicke’s area (dominant side): Language comprehension – lesion → receptive dysphasia.
- Memory, emotion (hippocampus, amygdala deep structures).
- Occipital lobe:
- Primary visual cortex (Brodmann 17): Calcarine sulcus, retinotopic mapping.
- Cuneus = upper retina, Lingual gyrus = lower retina.
- Visual association areas integrate images & interpretation.
- Insular cortex: Hidden in lateral fissure; roles in visceral sensation, autonomic control, emotion & addiction. Stroke sign: “loss of insular ribbon.”
Clinical Pearls
- Stroke: Knowing sulci helps localise lobar infarcts on CT/MRI (e.g. MCA territory → face/arm weakness + aphasia if dominant).
- Dementia: Alzheimer’s (temporal/parietal atrophy), FTD (frontal/temporal), PCA (occipital).
- Epilepsy: Focal seizures often map to cortical lobe of onset.
