
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Carpal tunnel syndrome
Related Subjects: |Tennis Elbow |Golfer's Elbow |Painful Shoulder syndromes |Plantar fasciitis |Carpal tunnel syndrome
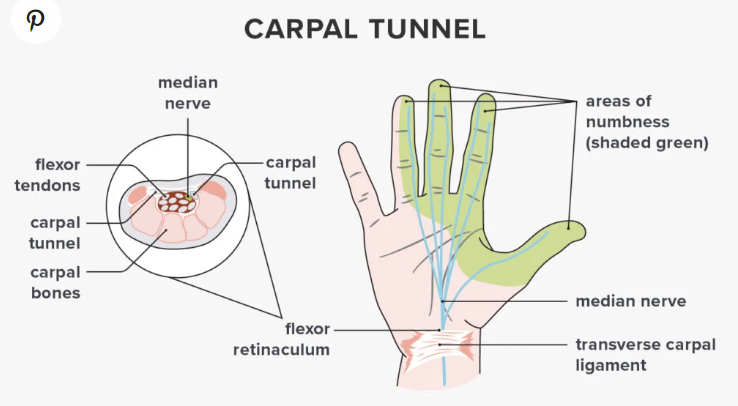
🖐️ Carpal tunnel syndrome (CTS) is the most common mononeuropathy, caused by compression of the median nerve within the carpal tunnel. It typically presents with nocturnal paraesthesia, hand pain, and sometimes thenar muscle weakness or wasting.
📌 About
- Most common entrapment neuropathy
- Median nerve compressed beneath the flexor retinaculum at the wrist
- Classically affects dominant hand, but can be bilateral
🧬 Aetiology
- Median nerve runs with 9 flexor tendons in the carpal tunnel → space-occupying or thickening processes lead to compression
- Can cause thenar wasting and impaired thumb opposition/abduction
- Weakness of abductor pollicis brevis and intrinsic hand muscles supplied by the median nerve
⚠️ Causes / Risk Factors
- Rheumatoid arthritis, pregnancy, acromegaly
- Colles’ fracture, minor trauma, idiopathic
- Amyloidosis (β2-microglobulin in dialysis patients)
- Myxoedema (hypothyroidism), obesity, diabetes
🩺 Clinical Features
- Paraesthesia and pain in radial 3½ fingers (thumb, index, middle, radial half of ring finger); palm sparing due to palmar cutaneous branch
- Nocturnal symptoms common; may radiate to forearm/shoulder
- Motor: thenar weakness, difficulty opposing thumb, thenar wasting late
- Provocative tests:
- 🔔 Tinel’s sign: percussion over flexor retinaculum → tingling
- 📐 Phalen’s test: forced wrist flexion 60 sec → symptoms reproduced

🔬 Investigations
- Bloods: FBC/U&E usually normal; TFT (hypothyroidism), B12 (neuropathy screen), ESR/protein studies if myeloma suspected
- Nerve conduction studies → delayed conduction across wrist (gold standard for diagnosis & severity grading)
- Needle EMG can show denervation if severe
🔎 Differentials
- Cervical radiculopathy (C6–C7): often with neck pain and dermatomal distribution
- Peripheral neuropathy (e.g. diabetic, B12 deficiency)
💊 Management
- 🔹 Treat underlying cause (e.g. hypothyroidism, inflammatory arthritis)
- 🔹 Splinting: neutral wrist splints, especially nocturnal
- 🔹 Analgesia ± corticosteroid injection into carpal tunnel (may cause transient worsening)
- 🔹 Surgery: carpal tunnel decompression (division of flexor retinaculum) if intractable symptoms, weakness, or NCS-confirmed severe disease
Cases - Carpal Tunnel Syndrome (CTS)
- Case 1 - Classic presentation ✋: A 48-year-old secretary reports tingling and numbness in the thumb, index, and middle fingers, worse at night and relieved by shaking her hand (“flick sign”). Exam: positive Tinel’s and Phalen’s tests. Diagnosis: idiopathic CTS. Managed with wrist splints and steroid injection if persistent.
- Case 2 - Secondary cause 🩺: A 36-year-old pregnant woman (third trimester) develops hand paraesthesia and nocturnal wrist pain. Exam confirms median nerve distribution sensory loss. Diagnosis: CTS secondary to fluid retention in pregnancy. Managed conservatively (splints, reassurance) as symptoms usually resolve postpartum.
- Case 3 - Severe disease 🔪: A 62-year-old man with type 2 diabetes presents with progressive numbness, thenar muscle wasting, and reduced grip strength. Nerve conduction studies: delayed median nerve conduction. Diagnosis: advanced CTS. Managed with surgical decompression (carpal tunnel release).
Teaching Point 🩺: CTS is due to median nerve compression in the carpal tunnel. Risk factors include diabetes, pregnancy, hypothyroidism, obesity, and repetitive wrist use. Early disease is often nocturnal and sensory; late disease causes motor weakness and thenar wasting. Nerve conduction studies confirm severity.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery