
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of Male Genitalia
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
The male genital system produces and delivers sperm and synthesises testosterone, enabling fertility, sexual function, and development of male secondary sexual characteristics. It is best understood as: (1) a testis that makes sperm + hormones, (2) a duct system that matures/transports sperm, (3) accessory glands that create seminal fluid, and (4) erectile and neuromuscular mechanisms that enable intercourse and ejaculation.
1) External Genitalia
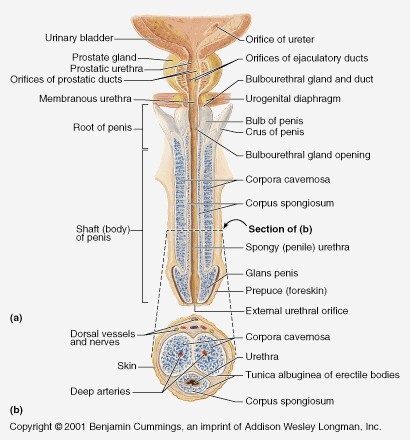
🍆 Penis - Structure, Erectile Tissues, and Urethra
The penis functions as a conduit for urine and semen and contains specialised erectile tissues that change rigidity with autonomic vascular control. An erection requires increased arterial inflow, reduced venous outflow, intact cavernosal smooth muscle relaxation, and appropriate neural signalling.
- Key parts:
- Root: bulb (corpus spongiosum) + crura (corpora cavernosa), anchored to perineal membrane.
- Body (shaft): contains erectile tissues and traversed by the urethra.
- Glans penis: expanded distal corpus spongiosum; highly innervated and sensitive.
- Prepuce (foreskin): retractable skin fold covering glans in uncircumcised males.
- Frenulum: ventral fold connecting prepuce to glans; rich sensory input.
- Erectile tissues:
- Corpora cavernosa (paired): main erectile bodies dorsally; responsible for rigidity.
– Enclosed by thick tunica albuginea which is crucial for the venous-occlusive mechanism. - Corpus spongiosum (single): surrounds urethra ventrally and expands to form the bulb and glans.
– Remains less rigid than cavernosa to prevent urethral compression during erection.
- Corpora cavernosa (paired): main erectile bodies dorsally; responsible for rigidity.
- Penile urethra: runs within corpus spongiosum; conducts urine and semen (not simultaneously).
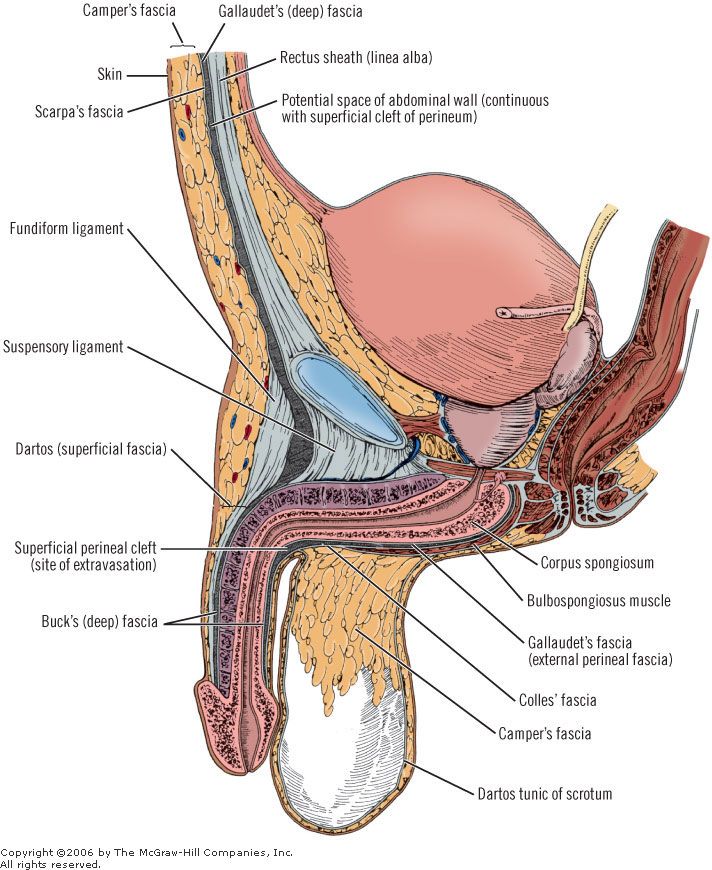
🧴 Scrotum - Protection and Temperature Control
The scrotum provides a cooler environment than core body temperature (typically ~2–4°C lower), which is essential for normal spermatogenesis. This is achieved by specialised muscle layers and a counter-current heat exchange system in the spermatic cord.
- Structure: skin + superficial fascia with dartos muscle (wrinkles scrotal skin, reducing heat loss when cold).
- Midline raphe: surface marker of embryological fusion; internal septum separates each testicular compartment.
- Cremaster muscle (from internal oblique; via spermatic cord): elevates testis when cold or during cremasteric reflex (important neuro exam).
- Pampiniform plexus: venous network that cools incoming arterial blood (counter-current heat exchange).
2) Internal Genitalia
🥚 Testes - Spermatogenesis and Testosterone Production
- Location: within scrotum; each testis is covered by:
- Tunica vaginalis (serous covering; derived from peritoneum).
- Tunica albuginea (tough fibrous capsule forming septa).
- Seminiferous tubules: site of spermatogenesis; lined by:
- Sertoli cells (supportive, endocrine, barrier functions).
- Developing germ cells (spermatogonia → spermatozoa).
- Interstitial (Leydig) cells: between tubules; synthesize testosterone in response to LH.
- Outflow: seminiferous tubules → straight tubules → rete testis → efferent ductules → epididymis.
🧪 Epididymis - Maturation and Storage
- Segments: head, body, tail (tail is main storage area).
- Role: sperm acquire motility and functional maturity; luminal environment modifies sperm membranes.
- Clinical: epididymitis commonly causes posterior testicular pain and swelling.
🚚 Vas Deferens (Ductus Deferens) - Transport “Pipe”
- Thick-walled muscular tube transporting sperm from epididymis tail to ejaculatory ducts.
- Travels in spermatic cord, through inguinal canal, into pelvis; crosses ureter (“water under the bridge”).
- Peristaltic contractions during emission propel sperm forward.
🧬 Seminal Vesicles, Prostate, Bulbourethral Glands - Semen Production
Semen is mostly glandular fluid; sperm are a minority by volume. Accessory gland secretions provide energy, buffering, and optimal viscosity to support sperm survival and motility.
- Seminal vesicles: produce fructose-rich, alkaline fluid + prostaglandins → energy and supportive medium.
– Contribute a large fraction of semen volume. - Prostate gland: produces thin, milky fluid containing enzymes (e.g., PSA) that help liquefy semen.
– Surrounds the proximal urethra; enlargement can obstruct urinary flow. - Bulbourethral (Cowper’s) glands: secrete clear mucus-like pre-ejaculate to lubricate urethra and neutralise residual acidity.
- Ejaculatory ducts: formed by union of vas deferens ampulla + seminal vesicle duct; open into the prostatic urethra.
3) Physiology
🧬 A) Spermatogenesis (Making sperm)
Spermatogenesis occurs in seminiferous tubules and takes ~2–3 months from spermatogonia to mature sperm. It requires a temperature slightly below core body temperature, adequate testosterone, FSH support, and intact Sertoli cell function.
- Key steps: spermatogonia → primary spermatocytes → secondary spermatocytes → spermatids → spermatozoa (spermiogenesis).
- Sertoli cells:
- Provide structural and metabolic support.
- Form the blood–testis barrier (tight junctions) → protects developing germ cells from immune attack and regulates microenvironment.
- Produce androgen-binding protein (ABP) to maintain high intratubular testosterone.
- Secrete inhibin B (negative feedback on FSH).
- During fetal life, produce anti-Müllerian hormone (AMH) to regress Müllerian ducts.
🧠 B) Hormonal Control (HPG axis)
- GnRH (hypothalamus) → stimulates pituitary release of LH and FSH.
- LH → stimulates Leydig cells → testosterone synthesis.
- FSH → acts on Sertoli cells → supports spermatogenesis and ABP production.
- Feedback: testosterone inhibits GnRH/LH; inhibin B inhibits FSH.
- DHT (from testosterone via 5α-reductase) is crucial for external genital development and contributes to prostate growth and hair patterns.
⚡ C) Erection (Neurovascular physiology)
An erection is primarily a parasympathetic event (“point”). Parasympathetic nerves release nitric oxide, increasing cGMP in cavernosal smooth muscle → relaxation, increased arterial inflow, and compression of subtunical veins (venous occlusion) to maintain rigidity.
- Parasympathetic (S2–S4, pelvic splanchnics): NO release → ↑ cGMP → smooth muscle relaxation.
- Arterial inflow: via deep arteries of penis → cavernosal spaces fill.
- Venous occlusion: tunica albuginea compresses venules → reduced outflow.
- Drug link: PDE5 inhibitors (e.g., sildenafil) prevent cGMP breakdown → enhance erection (require sexual stimulation/NO release).
💥 D) Emission and Ejaculation
Emission is mainly sympathetic (“shoot”), moving semen into the posterior urethra; ejaculation is a coordinated reflex involving somatic and autonomic pathways causing rhythmic contractions of pelvic muscles and urethral expulsion.
- Emission (sympathetic): vas deferens, seminal vesicles, prostate contract → semen enters prostatic urethra; bladder neck contracts to prevent retrograde flow.
- Ejaculation (somatic + autonomic): rhythmic contraction of bulbospongiosus and pelvic floor (pudendal nerve) expels semen.
🩸 Blood Supply, Innervation & Lymphatics
🩸 Blood Supply
- Penis/scrotum: mainly via internal pudendal artery (internal iliac branch) → deep and dorsal arteries of penis.
- Testes: testicular arteries arise directly from the abdominal aorta (high-yield).
- Venous drainage:
- Pampiniform plexus → testicular veins (left often drains to left renal vein; right to IVC).
- Penile venous drainage via deep dorsal vein → prostatic plexus.
🧠 Innervation
- Somatic: pudendal nerve (S2–S4) supplies sensory innervation (glans/skin) and motor to perineal muscles (e.g., bulbospongiosus).
- Autonomic:
- Parasympathetic (S2–S4): erection.
- Sympathetic (T11–L2): emission, bladder neck closure, detumescence.
🌿 Lymphatic Drainage (Very high-yield)
- Testes: drain to para-aortic (lumbar) nodes (reflects embryological origin in abdomen).
- Scrotal skin: superficial inguinal nodes.
- Penis:
- Skin/shaft mainly → superficial inguinal.
- Glans and deeper structures often → deep inguinal and external iliac.
🧫 Embryology (Brief but Clinically Useful)
- Genital tubercle → penis (glans and shaft structures).
- Urogenital folds → ventral penile urethra.
- Labioscrotal swellings → scrotum.
- Testicular descent: testes form near kidneys and descend via inguinal canal guided by gubernaculum; failure → cryptorchidism (fertility and malignancy risk).
⚕️ Clinical Correlations
- Congenital anomalies
- Hypospadias: urethral meatus on ventral shaft/glans; associated with chordee; surgical repair often required.
- Cryptorchidism: undescended testis → impaired spermatogenesis and increased testicular cancer risk if not corrected.
- Testicular torsion: acute scrotal pain; time-critical surgical emergency (spermatic cord twist compromises arterial flow).
- Infections/inflammation
- Epididymo-orchitis: often bacterial/STI; pain, swelling; consider torsion in acute presentations.
- Prostatitis: pelvic pain, LUTS, systemic features; can cause urinary retention.
- Balanitis: glans inflammation; hygiene, diabetes, Candida considerations.
- Neoplasia
- Testicular cancer: painless lump; spreads to para-aortic nodes; excellent cure rates if treated early.
- Prostate cancer: may be asymptomatic early; LUTS more commonly benign prostatic enlargement.
- Penile cancer: related to HPV and chronic inflammation; lymphatic spread to inguinal nodes.
- Functional disorders
- Erectile dysfunction: vascular, neurogenic, endocrine, psychogenic, medication-related; often a marker of cardiovascular risk.
- Infertility: may reflect spermatogenic failure, obstruction, endocrine causes, varicocele, or systemic disease.
✅ Conclusion
The male genital system combines hormone production (testosterone), sperm generation (seminiferous tubules), maturation/storage (epididymis), transport (vas deferens and ducts), and seminal fluid support (seminal vesicles, prostate, bulbourethral glands). Neurovascular control coordinates erection (parasympathetic) and emission/ejaculation (sympathetic + somatic). High-yield anatomy includes lymphatic drainage (testes → para-aortic; scrotum → superficial inguinal) and the time-critical nature of torsion and obstructive pathology.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery