
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Fractured Neck of Femur/Femoral Neck
Related Subjects: |Fractured Neck of Femur |Fractured Shaft Femur |Supracondylar Femur Fractures |Femoral fractures and Injuries
⚠️ Key Point: Intracapsular fractures have a higher incidence of AVN (Avascular Necrosis) and non-union due to the femoral head blood supply. 👉 If displacement is minimal → internal fixation gives best outcome. 👉 If displaced → high risk of AVN, so prosthesis insertion usually a hemiarthroplasty or a total hip replacement to replace the femoral head is usually required.
ℹ️ About
- 🦴 Intracapsular fractures carry high AVN risk.
- ☠️ 30% of patients die within 1 year.
- 👵 Most common in the elderly due to frailty and falls.
- 🧓 Patients often have multiple co-morbidities.
- 🦴 Osteoporosis is the major underlying factor.
📊 Epidemiology
- ~80,000 hip fractures per year in the UK.
- Numbers are rising as the population ages.
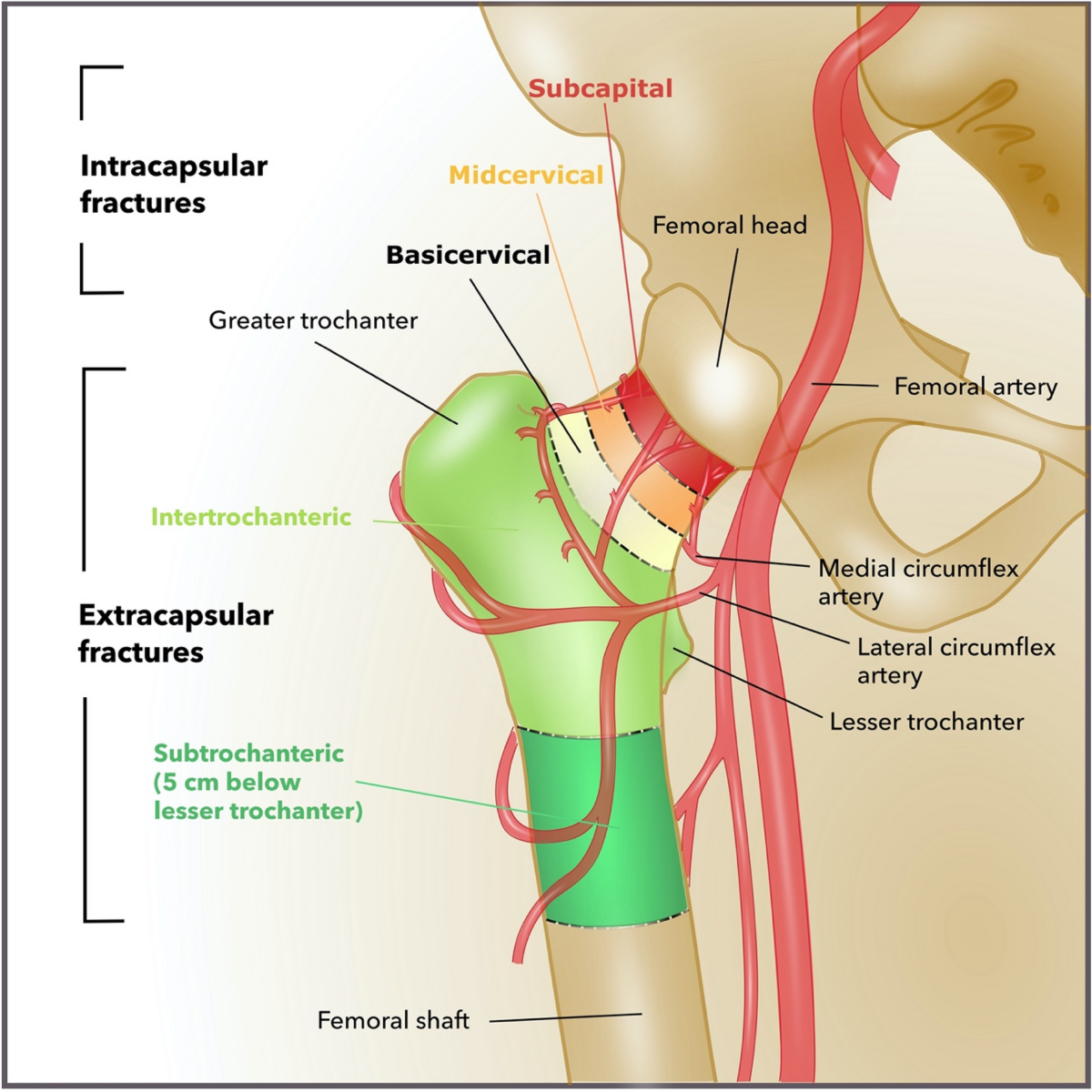
🧠 Anatomy
🧬 Aetiology
- Falls + Osteoporosis are the commonest causes.
- The medial femoral circumflex artery supplies the femoral head ➝ vulnerable in NOF fractures.
- Vascular compromise ➝ ischaemia ➝ AVN.
📉 Risk Factors for Bone Fragility
- Osteoporosis: age, inactivity, smoking, alcohol, low BMI, family history.
- Previous fragility fracture ➝ doubles future fracture risk.
- Other causes: metastases, Paget’s disease, osteomalacia, hyperparathyroidism, myeloma.
🤕 Risk Factors for Falls
- Muscle weakness, gait or balance problems.
- Neurological diseases: Parkinson’s, stroke.
- Poor vision.
- Medications: sedatives, hypnotics, diuretics, antihypertensives, alcohol.
🩺 Clinical Features
- Pain + external rotation, adduction, and shortening of the affected leg.
- History: establish whether mechanical fall or medical cause (syncope, arrhythmia, hypotension).
- Check co-morbidities that influence management.
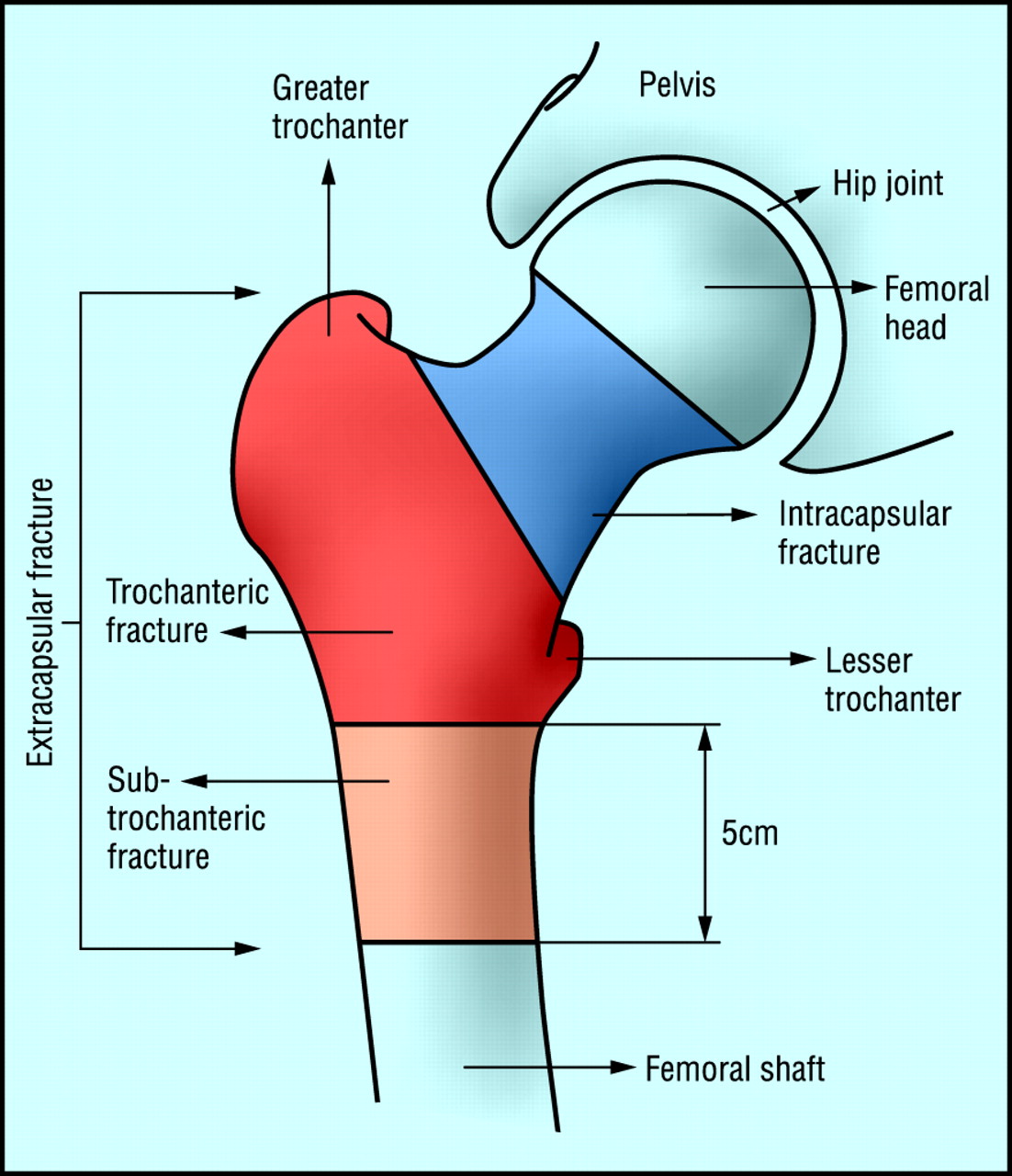
📌 Types of Fracture
- Intracapsular: High risk of AVN + non-union. Tx = hemiarthroplasty/THR.
- Subcapital & Transcervical: Common intracapsular fracture patterns.
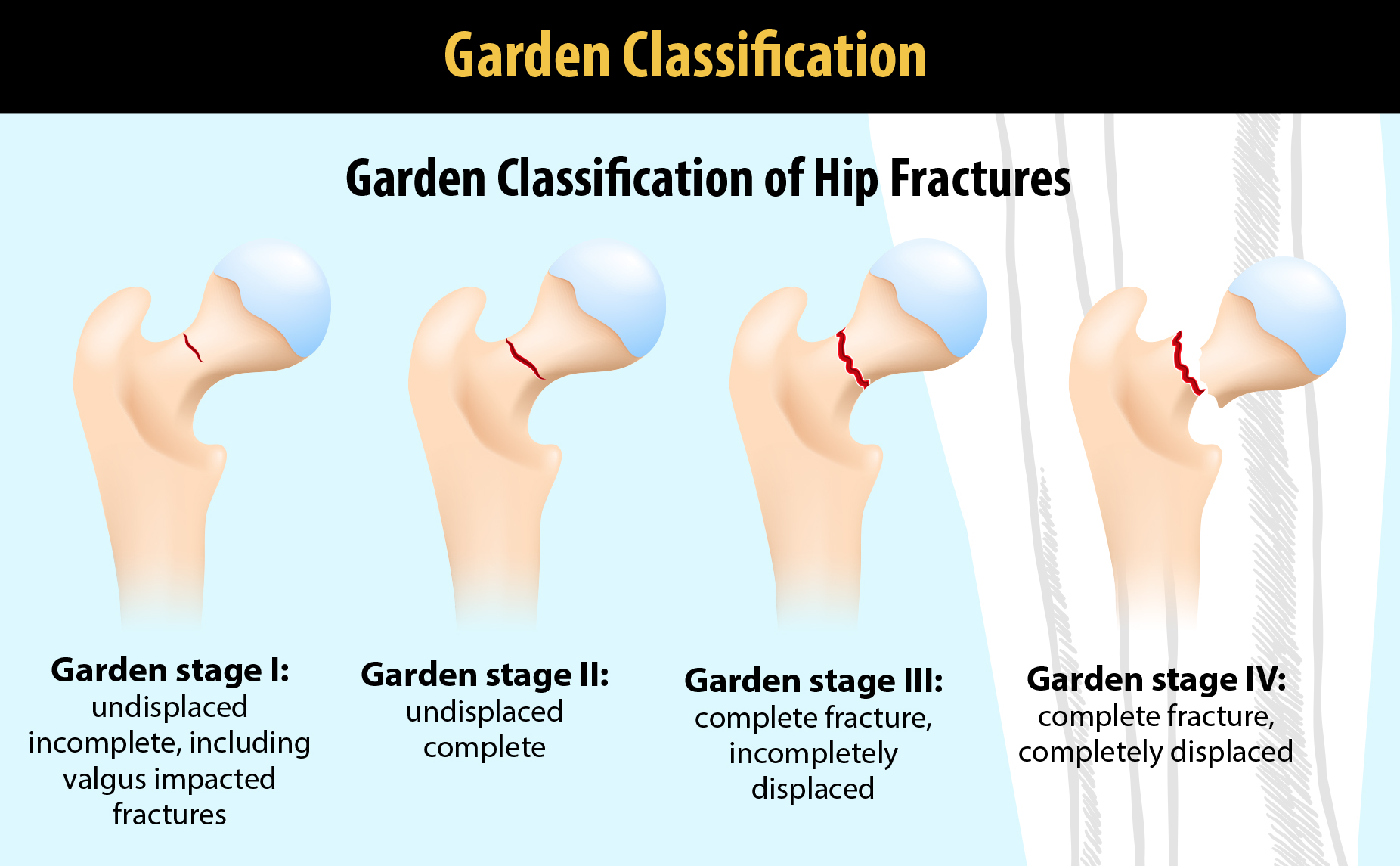
🗂️ Garden Classification
- Type I: Incomplete fracture
- Type II: Complete, undisplaced
- Type III: Complete, partially displaced
- Type IV: Complete, fully displaced
📌 Extracapsular Fractures
- Trochanteric
- Transtrochanteric
- Subtrochanteric
Other Fractures
- Pubic ramus fractures (usually conservative).
- Acetabular fractures (conservative unless complex).
🔍 Investigations
- Baseline bloods: FBC, U&E, clotting, group & save.
- CXR + ECG (pre-op assessment).
- Pelvic AP X-ray (compare both hips, check pubic rami).
- Lateral hip X-ray (often diagnostic when AP is normal).
- MRI/CT if X-rays inconclusive (10% occult fractures).
🛡️ Prevention
- Falls risk assessment + home/environment modifications.
- Muscle strengthening + balance retraining (e.g. Tai Chi).
- Bisphosphonates increase bone density, reduce fracture risk.
- Calcium, Vitamin D, ± HRT can reduce risk.
📊 Mortality: 10% at 30 days, 30% at 12 months (reflecting frailty + co-morbidities).
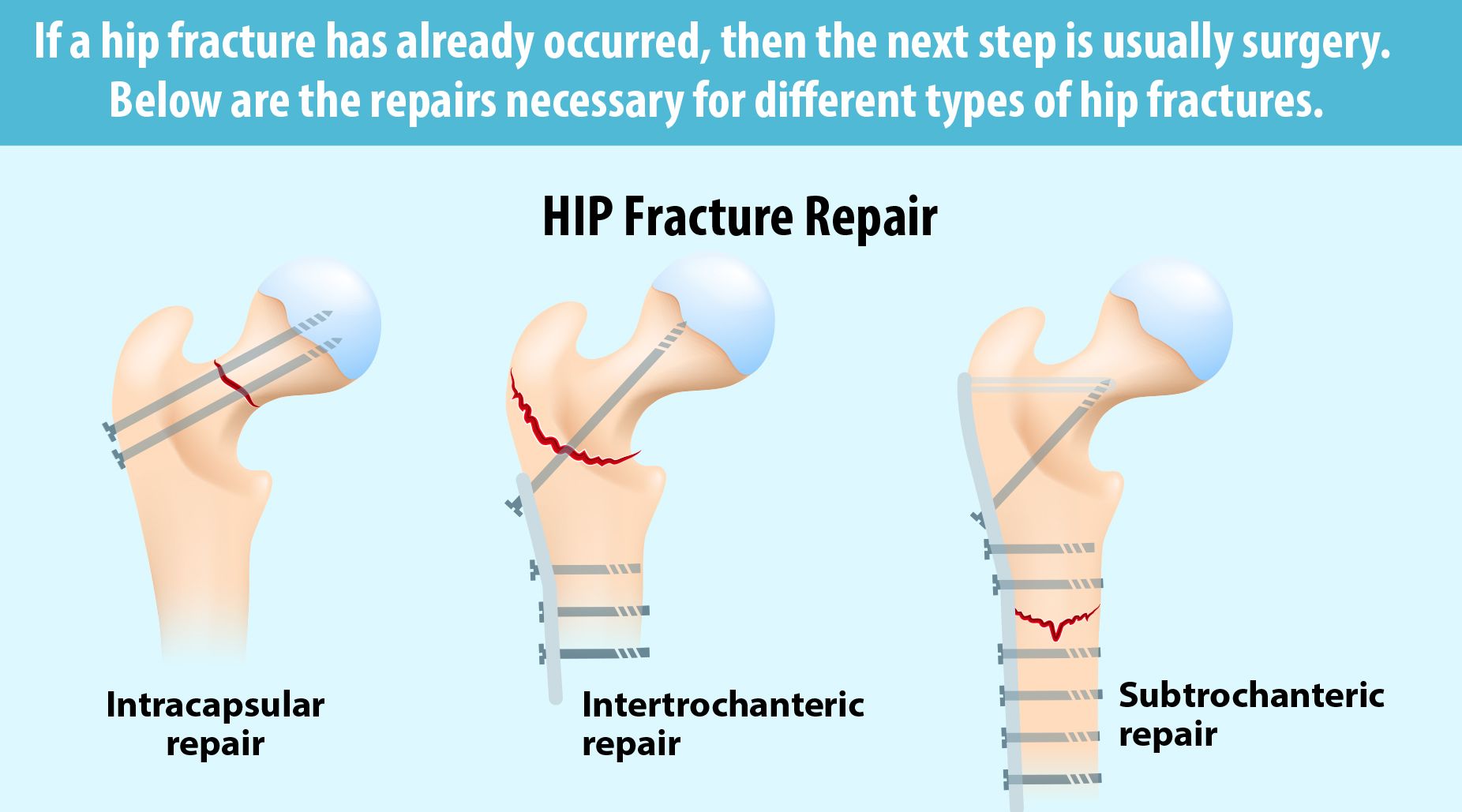
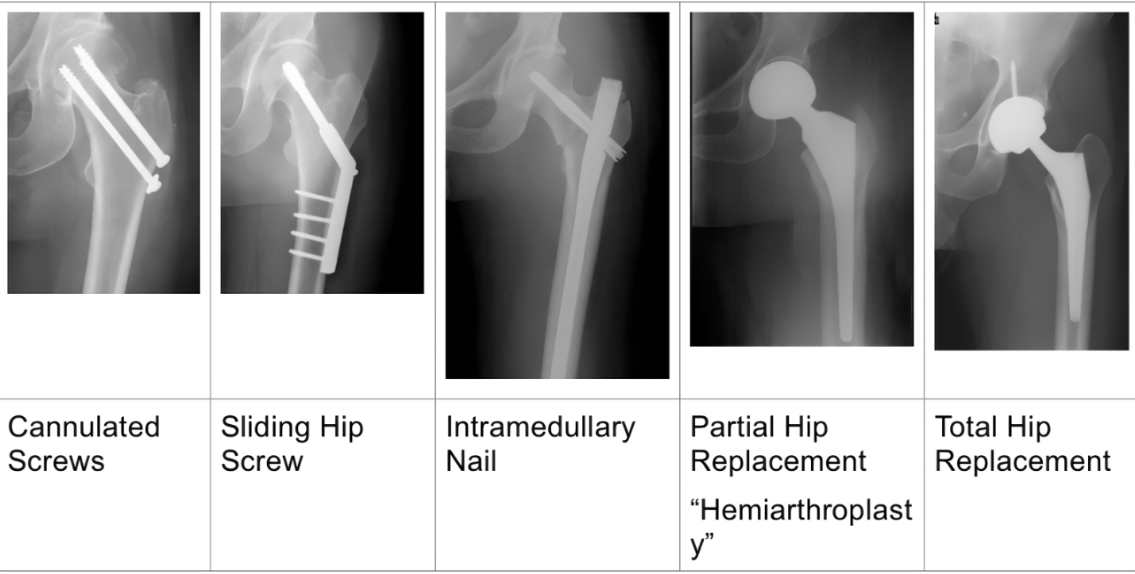
🛠️ Treatment Options
- Conservative: For patients unfit for surgery ➝ bed rest, analgesia, physio. Poor outcomes.
- Surgical: Standard of care.
- Internal fixation: For undisplaced intracapsular (cannulated screws/DHS). Also for young with displaced fractures.
- Hemiarthroplasty: For older patients with displaced fractures ➝ faster recovery.
- Total Hip Replacement (THR): For active elderly/younger displaced fractures ➝ better function long term, higher surgical risk.
- Intramedullary nailing: For extracapsular/subtrochanteric fractures ➝ early mobilisation.
- DHS: For intertrochanteric fractures ➝ controlled collapse and healing.
In frail elderly after a hip fracture, annual IV zoledronate not only prevents further fractures but also reduces mortality. This is unique among osteoporosis treatments and why geriatricians are so keen to give it post-fracture. 5 mg IV once yearly, infused over at least 15 minutes. Ensure adequate vitamin D and calcium before infusion (correct hypocalcaemia). The evidence was in groups with mean age of 75 so may not apply to much older patients.
🩺 Management
- ABC resuscitation.
- Analgesia (including fascia iliaca block).
- IV fluids & electrolyte correction.
- Orthogeriatric review early.
- Admit + imaging if unable to walk or occult fracture suspected.
- Assess mental state, pressure sore risk, nutrition.
- Surgery:
- Intracapsular undisplaced ➝ cannulated screws.
- Intracapsular displaced ➝ hemiarthroplasty or THR if fit.
- Extracapsular ➝ screws/nailing depending on pattern.
- VTE prophylaxis ➝ stockings + LMWH/DOAC until mobilising.
🏃♀️ Post-Surgical Care & Rehabilitation
- Early mobilisation with physio ➝ prevents DVT, improves outcomes.
- Pain management + infection prophylaxis.
- Monitor for complications: infection, non-union, prosthetic dislocation.
- Rehab programmes: strength, balance, gait training ➝ reduce future falls.
⚠️ Complications
- AVN (esp. intracapsular fractures).
- Non-union (esp. displaced fractures).
- Osteoarthritis.
- DVT/PE.
- Surgical site infection, prosthetic dislocation.
📈 Prognosis
- Outcome depends on age, co-morbidities, and rapidity of surgery.
- Mortality: ~30% at 1 year, largely due to frailty not fracture itself.
- Good surgical + rehab care ➝ mobility and independence can be maintained.
✅ Conclusion
Fractured neck of femur is a major orthopaedic emergency, common in elderly patients with osteoporosis and falls. Intracapsular fractures are particularly high risk due to compromised blood supply ➝ AVN + non-union. Prompt surgical management (fixation or replacement), multidisciplinary orthogeriatric input, and effective rehab are key to improving survival and function.
📚 References
- Royal College of Physicians – Fractured Neck of Femur
- NICE – Hip Fracture Management Guidelines
- Mayo Clinic – Hip Fracture
- UpToDate – Hip Fracture Overview
- British Orthopaedic Association – Hip Fracture Guidance
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery