Related Subjects:
| High Altitude Physiology
| Diving Physiology
| Trauma Physiology
| Exercise Physiology
| Gastric Physiology
| Rectal Physiology
What is Diving Physiology? ⚓🐠
Diving physiology explains how the body responds to increased pressure, denser breathing gases, immersion, and cold. Understanding these changes is essential for safe diving and for recognising and treating dive-related illness.
Core Physics Underwater 🧮
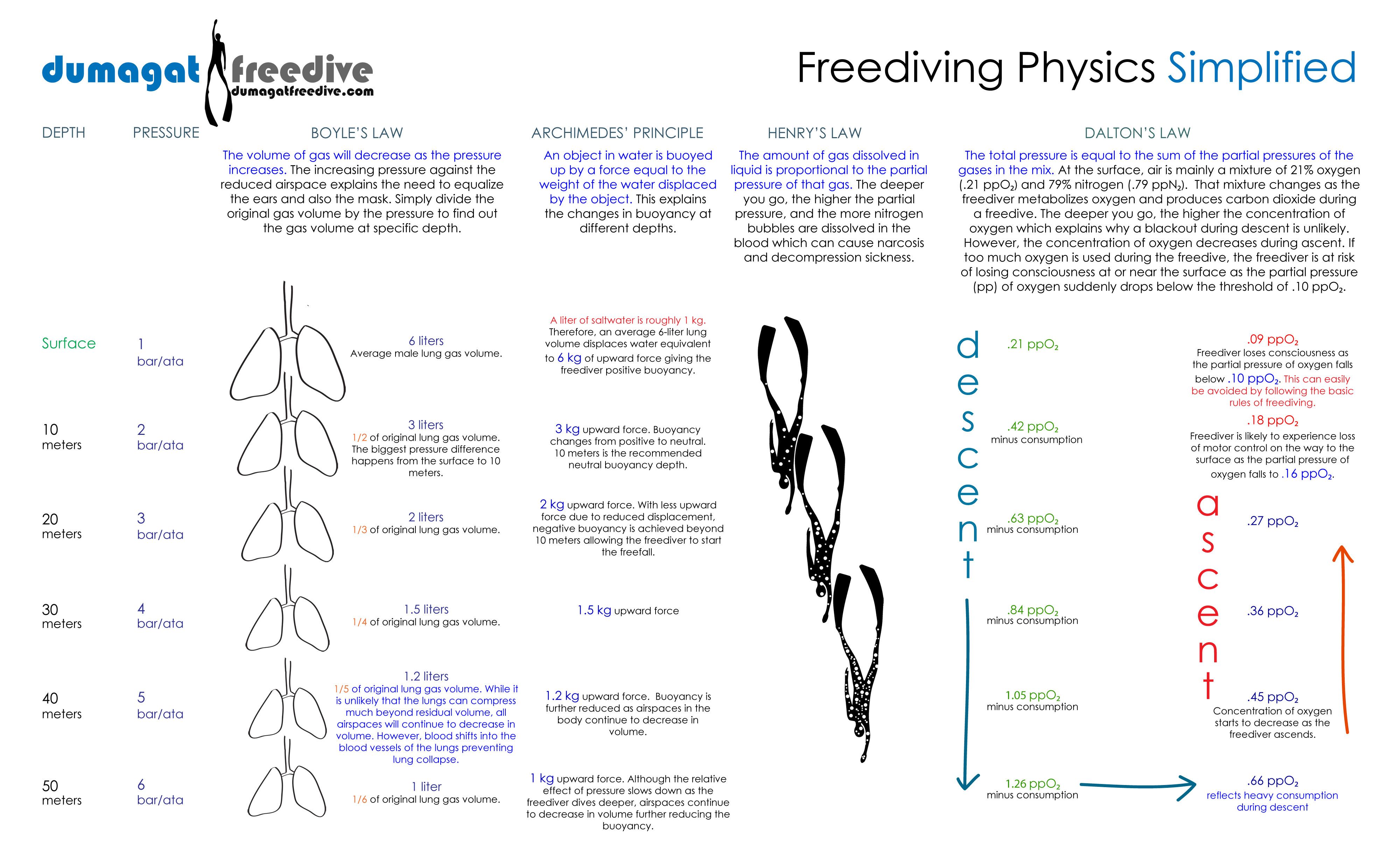
- Pressure & Depth: In seawater, pressure increases ~1 atmosphere (atm) every 10 m (33 ft). Surface = 1 atm; 30 m ≈ 4 atm.
- Boyle’s law (P×V = constant): As pressure increases, gas volume decreases (lungs, mask, middle ear) → equalise early & often.
- Dalton’s law: Partial pressure of each gas = fraction × total pressure. At depth, rising ppO2 and ppN2 drive oxygen toxicity and narcosis risk.
- Henry’s law: Dissolved gas ∝ partial pressure. More nitrogen dissolves at depth; too-rapid ascent forms bubbles → decompression sickness (DCS).
- Gas density & work of breathing 🫁: Denser gas at depth increases resistance; risk of CO2 retention during exertion.
Physiological Responses to Immersion 🌊
- Mammalian diving reflex:
- Vagal bradycardia ❤️ conserves oxygen
- Peripheral vasoconstriction preserves cerebral/cardiac perfusion
- Blood shift toward the thorax at depth protects alveoli (notably in breath-hold diving)
- Immersion & cold:
- ↑ Central blood volume → diuresis (cold water diuresis) → dehydration risk 💧
- Cold stress → shivering, ↑ O2 consumption; fine-motor decline and afterdrop on exit
Lungs & Ventilation Under Pressure 🫁
- Lung volumes: Gas compression reduces volume; breath-hold descent risks “lung squeeze”.
- Work of breathing: Dense gas, tight suit, regulator load → hypercapnia risk (headache, dyspnoea, panic).
- V/Q changes: Hydrostatic gradients and post-dive microbubbles can increase dead space and alter gas exchange.
Breathing Gas Options 🔬
- Air: 21% O2 / 79% N2. Simple, but depth limited by narcosis and ppO2.
- Nitrox (EANx): ↑ O2, ↓ N2 → less N2 loading and longer NDLs; respect ppO2 limits (typical working ≤1.4 ata).
- Trimix: Adds helium to reduce narcosis and gas density for deep dives; monitor HPNS and thermal loss.
- Heliox: Helium + O2, used for very deep/commercial dives; minimal narcosis, low density.
Diving-Related Illnesses & Injuries 🚑
Barotrauma (Boyle’s Law–Driven)
| Site |
Mechanism & Features |
Prevention / First Aid |
| Middle ear / sinuses 👂 |
Failure to equalise on descent → pain, haemotympanum; on ascent → reverse block |
Equalise early/often; stop descent if pain; avoid diving with URTI |
| Lungs |
Breath-holding on ascent → alveolar rupture, pneumothorax, mediastinal emphysema, arterial gas embolism (AGE) |
Never hold breath; controlled ascent; 100% O2 and urgent evaluation if chest pain/neurology |
| Mask / suit / dental |
Mask squeeze (periorbital petechiae), suit squeeze; trapped gas under fillings |
Exhale via nose into mask; proper fit; dental issues addressed pre-dive |
Decompression Sickness (DCS) “The Bends”
- Cause: Inert gas (usually nitrogen) coming out of solution as bubbles during/after ascent.
- Type I: Joint/limb pain, pruritus, skin marbling (cutis marmorata), lymphatic swelling.
- Type II: Neurologic deficits, ataxia/vertigo, pulmonary “chokes”, spinal cord syndromes.
- Immediate actions: 100% O2, supine, hydrate if able, minimise exertion; arrange hyperbaric recompression ASAP.
- Prevention: Conservative profiles, slow ascents, safety stops, adequate surface intervals, hydration, avoid heavy exertion post-dive, respect “no-fly” intervals.
Arterial Gas Embolism (AGE)
- Mechanism: Over-expansion injury → alveolar rupture → gas enters arterial circulation → stroke-like symptoms within minutes of ascent.
- Management: 100% O2, airway protection, rapid evacuation for recompression.
Nitrogen Narcosis 🤿
- Features: Euphoria, poor judgement, tunnel vision, slowed reactions (often >30 m on air; dose-dependent with depth).
- Prevention: Limit depth; use helium mixes for deeper dives; ascend if symptomatic.
Oxygen Toxicity (ppO2 too high) 🧯
- CNS toxicity: Visual/auditory changes, nausea, twitching, seizures (risk ↑ with ppO2 ≥1.6 ata, CO2 retention, cold, stress).
- Pulmonary toxicity: With prolonged high FiO2 exposure → cough, chest tightness, ↓ vital capacity.
- Mitigation: Respect ppO2 limits (work ≤1.4 ata; deco ≤1.6 ata), manage workload/CO2, limit exposure time.
CO2 Retention & Work of Breathing
- Causes: Dense gas at depth, heavy exertion, inadequate ventilation, rebreather scrubber failure.
- Symptoms: Headache, dyspnoea, anxiety/panic, confusion; potentiates O2 toxicity & narcosis.
- Action: Reduce exertion, improve ventilation, change depth/gas per training; abort if unresolved.
Hypothermia & Thermal Stress ❄️
- Water conducts heat ~25× faster than air → major heat loss risk.
- Prevention: Appropriate wet/dry suit, hood, gloves; nutrition/hydration; warm-up between dives.
Breathing Gas Mixtures
- Nitrox: Higher O2 than air; reduces N2 uptake and DCS risk; monitor ppO2 carefully.
- Trimix: N2 + O2 + He; reduces narcosis and gas density for deep/technical dives.
- Heliox: He + O2; used in deep commercial/medical operations to minimise narcosis and density.
Dive Planning & Safety 🧭
- Dive tables & computers: Plan bottom time, ascent rate, safety/decompression stops; remain within training.
- Ascent discipline: Typical ≤9–10 m/min; add 3–5 min safety stop at 3–5 m when appropriate.
- Buddy system 👥: Pre-dive checks (e.g., BWRAF), gas planning (e.g., rule of thirds), lost-buddy protocol.
- Emergency skills: Controlled emergency swimming ascent (CESA), SMB deployment, rescue towing, 100% O2 first aid.
Research & Future Directions 🔭
- Refined decompression algorithms (bubble models, personalised risk scoring).
- Lower-density gases and improved rebreather scrubbers to mitigate CO2 retention.
- Wearables tracking thermal status and perfusion to prevent hypothermia and DCS.
Summary
Diving physiology explores the body’s adaptations to underwater pressure, gas partial pressures, and cold. Key risks-barotrauma, DCS/AGE, narcosis, oxygen toxicity, CO2 retention, and hypothermia-are largely preventable with prudent dive planning, correct gas choice, disciplined ascent rates, thermal protection, and early use of 100% oxygen when problems arise. 🧡
