
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Liver
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen |AP of the Liver
🫀 AP of the Liver (with Drug Metabolism + Paracetamol)
The liver is the body’s central metabolic and detoxification hub. Clinically, many problems map to: hepatocellular injury (ALT/AST), cholestasis (ALP/GGT), or synthetic/metabolic failure (INR, albumin, glucose, ammonia), often alongside portal hypertension as fibrosis advances.
🧬 Introduction
- The liver weighs ~1.2–1.5 kg and performs hundreds of essential functions: metabolism, synthesis, storage, bile production, and detoxification.
- It lies mainly in the right upper quadrant beneath the diaphragm; pain is typically from capsular stretch (Glisson’s capsule), not hepatocytes themselves.
- Segmental anatomy (Couinaud segments) allows targeted resection and transplantation planning.
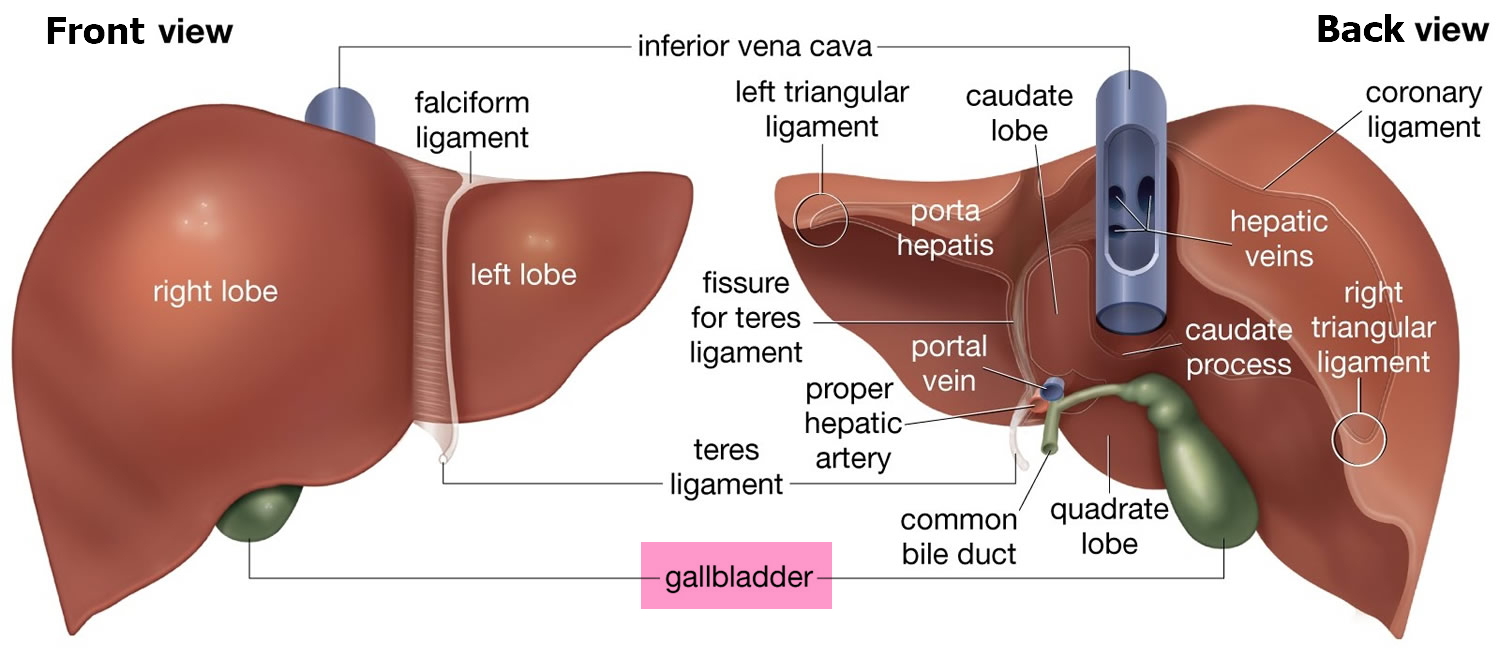
📍 Gross Anatomy and Couinaud Segments
Surface anatomy describes right and left lobes (falciform ligament). Functionally, the liver has 8 Couinaud segments, each with its own portal inflow, venous outflow, and biliary drainage.
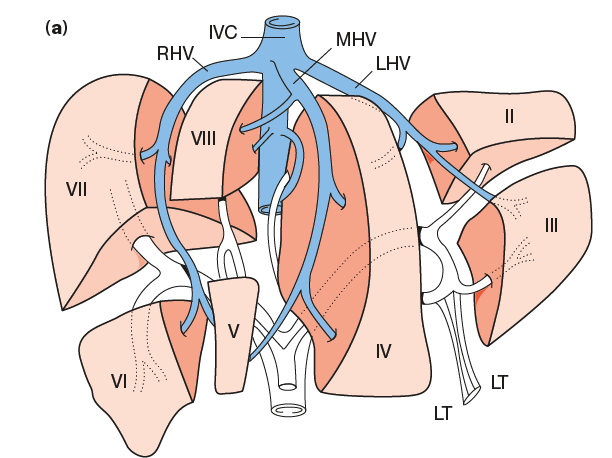
- I: Caudate (independent inflow; drains directly to IVC; can hypertrophy in cirrhosis).
- II–III: Left lateral (superior/inferior).
- IVa–IVb: Left medial (superior/inferior).
- V–VIII: Right lobe (anterior/posterior; inferior/superior).
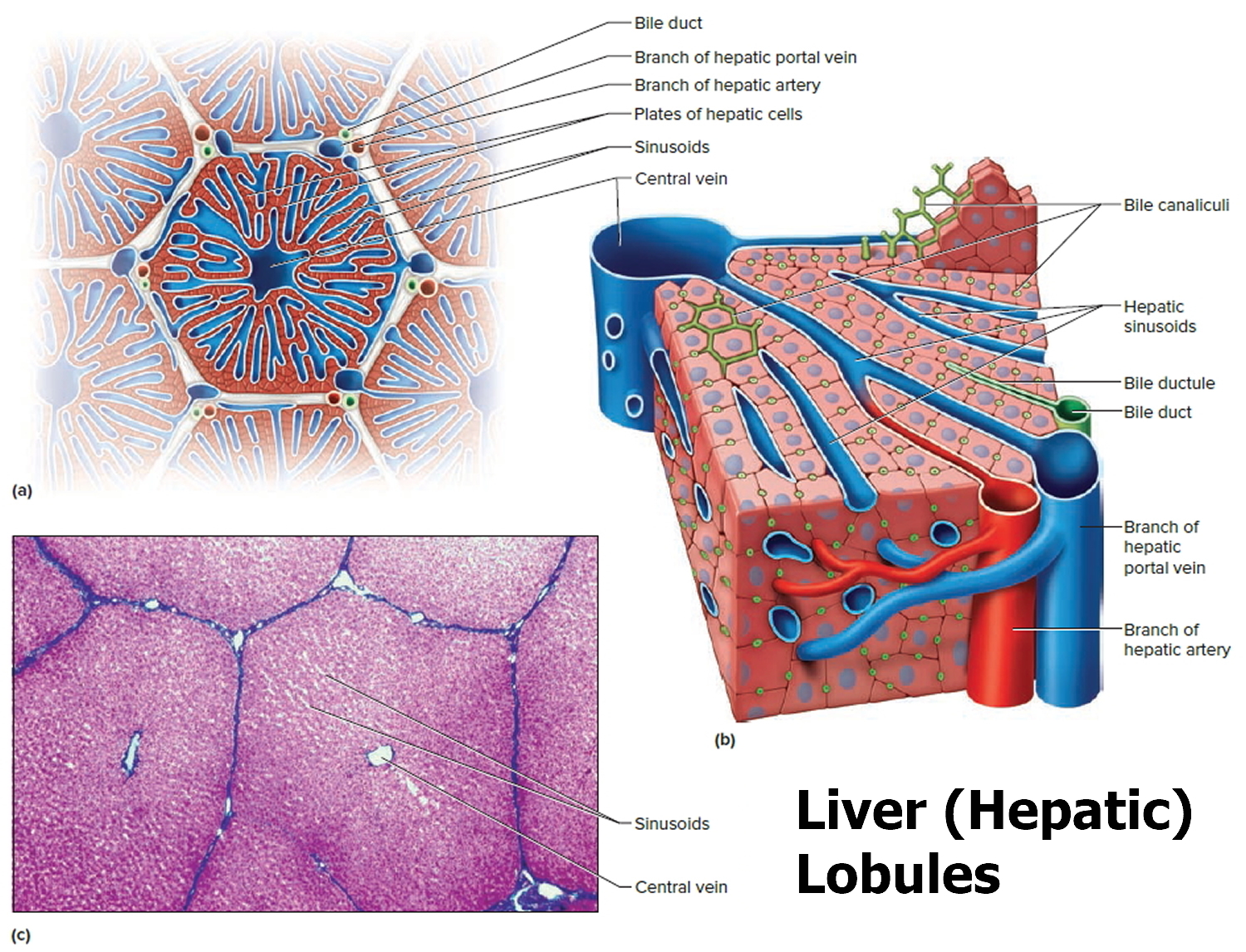
🔬 Microscopic Anatomy (functional microcirculation)
- Lobule: Hepatocyte plates draining to a central vein.
- Portal triad: Portal venule + hepatic arteriole + bile ductule at the periphery.
- Sinusoids: Fenestrated vessels enabling rapid exchange (nutrients, drugs, toxins).
- Kupffer cells: Macrophages filtering portal blood (bacterial/endotoxin clearance).
- Space of Disse: Exchange interface; lymph formation site.
- Stellate cells: Store vitamin A; activation → collagen deposition → fibrosis/cirrhosis.
Fibrosis begins when stellate cells activate → collagen in the Space of Disse → sinusoidal “capillarisation” → reduced exchange + increased portal resistance (portal hypertension).
💉 Blood Supply and Portal Flow
- Portal vein (~75% flow): nutrient-rich blood from gut/spleen; delivers absorbed drugs/toxins first (first-pass effect).
- Hepatic artery (~25% flow): oxygen-rich blood from coeliac axis.
- Outflow: hepatic veins → IVC.
🟡 Bile Production and Flow
- Bile flows from hepatocytes → canaliculi → ducts → hepatic ducts → common hepatic duct → CBD → duodenum.
- Bile acids emulsify fats and enable absorption of fat-soluble vitamins (A, D, E, K); conjugated bilirubin is excreted via bile.
🗺️ Acinar Zonation (why injury patterns differ)
- Zone 1 (periportal): highest oxygen and nutrients; first exposed to portal blood (including some toxins).
- Zone 2: intermediate.
- Zone 3 (centrilobular): lowest oxygen but highest CYP450 activity → most vulnerable to hypoxic injury and reactive drug metabolites (classically paracetamol).
Zone 3 sits “furthest” from oxygenated inflow and is CYP450-rich - perfect setup for ischaemic hepatitis (shock liver) and toxic-metabolite injury.
⚙️ Liver Physiology - Expanded and Clinically Useful
🍞 Carbohydrate Handling
- Fed state: insulin-driven glycogenesis (glucose → glycogen).
- Fasting: glucagon/adrenaline-driven glycogenolysis (glycogen → glucose).
- Prolonged fasting/illness: gluconeogenesis from lactate (Cori cycle), glycerol, and amino acids.
- Clinical: severe liver failure → impaired gluconeogenesis → hypoglycaemia, especially in sepsis/alcohol misuse.
🧈 Lipid Handling
- Synthesises cholesterol (precursor for steroid hormones + bile acids).
- Packages triglycerides into VLDL for export; handles HDL pathways.
- β-oxidation produces energy; ketogenesis supports fasting physiology.
- Clinical: insulin resistance → hepatic triglyceride accumulation → MASLD/NAFLD.
🥚 Protein and Nitrogen Handling
- Synthesises albumin (oncotic pressure + drug binding) and many transport proteins.
- Synthesises clotting factors (II, VII, IX, X) and regulators (protein C/S) → explains raised INR in liver failure.
- Urea cycle converts ammonia to urea (prevents neurotoxicity).
- Clinical: impaired ammonia clearance → astrocyte swelling + neurotransmitter imbalance → hepatic encephalopathy.
🛡️ Immunology and Inflammation
- Kupffer cells filter portal blood, clearing bacteria/endotoxin (key barrier to gut translocation).
- Liver produces acute phase proteins (e.g. CRP) and complement components.
- Clinical: cirrhosis = immune dysfunction (susceptibility to infections like SBP).
💊 Drug Handling and Hepatic Biotransformation (very high-yield)
Most drugs are either metabolised in the liver, excreted in bile, or both. Hepatic handling depends on: hepatic blood flow, protein binding, intrinsic metabolic capacity, and biliary transport. Cirrhosis reduces functional hepatocyte mass and distorts microcirculation, so drug effects become unpredictable.
🏭 First-pass metabolism (why oral doses behave differently)
- Drugs absorbed from the gut enter the liver via the portal vein before reaching systemic circulation.
- High first-pass drugs can have low oral bioavailability; liver disease may increase bioavailability → higher plasma levels at “usual” doses.
- Examples (conceptual): some opioids, beta-blockers, nitrates, and calcium channel blockers have significant first-pass effects (drug-specific).
🧪 Phase I and Phase II metabolism
- Phase I (CYP450): oxidation/reduction/hydrolysis → may create reactive intermediates (important in toxicity).
- Phase II (conjugation): glucuronidation, sulphation, acetylation, methylation, glutathione conjugation → makes compounds water-soluble and safer for excretion.
- Cholestasis can impair biliary excretion → drug accumulation (especially with biliary elimination).
🔁 What changes in liver disease (practical prescribing physiology)
- ↓ Albumin → ↑ free fraction of highly protein-bound drugs (more effect/toxicity at same total level).
- Portosystemic shunting reduces first-pass clearance → oral doses behave “stronger”.
- ↓ CYP activity (variable) + ↓ hepatocyte mass → slower clearance for many drugs.
- Cholestasis → reduced biliary excretion.
- Ascites/edema → increased volume of distribution for hydrophilic drugs (complex dosing effects).
✅ Rule of thumb: in decompensated cirrhosis, start low, go slow, reassess frequently, and avoid hepatotoxic medicines where possible. Always consider renal function too (hepatorenal physiology).
🚑 Paracetamol (Acetaminophen) - Physiology of Toxicity
Paracetamol is usually safe at therapeutic doses because most is metabolised by glucuronidation and sulphation (Phase II pathways). A small fraction is metabolised via CYP450 (especially CYP2E1) to a reactive metabolite called NAPQI. NAPQI is normally detoxified by glutathione.
- Normal dose: conjugation pathways dominate; minimal NAPQI; glutathione easily neutralises it.
- Overdose: conjugation pathways saturate → more paracetamol diverted to CYP450 → excessive NAPQI → glutathione depletion → NAPQI binds hepatocyte proteins → oxidative injury and cell death.
- Where? Injury is typically centrilobular (Zone 3) due to high CYP activity and low oxygen reserve.
⚠️ Who is at higher risk of toxicity at lower doses?
- Chronic alcohol use (induces CYP2E1; may reduce glutathione stores).
- Malnutrition / fasting (reduced glutathione precursor availability).
- Enzyme-inducing drugs (some antiepileptics; depends on agent).
- Chronic liver disease (risk depends on reserve and nutrition; dosing must be cautious and individualised).
🧯 Why NAC works (mechanism, not just “because guidelines say so”)
- N-acetylcysteine (NAC) replenishes glutathione stores and provides sulphydryl groups to detoxify NAPQI.
- It also improves microcirculatory blood flow and acts as an antioxidant, which helps even when presentation is delayed.
Paracetamol toxicity is a classic example of liver physiology: Phase II saturation + Zone 3 CYP activity + glutathione depletion → predictable injury pattern. This is why timing, risk factors, and early antidote matter.
🩺 Clinical Relevance (how physiology shows up)
- Shock liver (ischaemic hepatitis): profound hypotension/hypoxia → marked ALT/AST rise; Zone 3 vulnerability.
- Cholestasis: pruritus + ALP/GGT rise; drug accumulation if biliary elimination impaired.
- Hepatic encephalopathy: ammonia and neurotoxin handling failure; precipitated by infection, GI bleed, constipation, sedatives.
- Cirrhosis: synthetic failure (INR, albumin), portal hypertension (varices/ascites), immune dysfunction.
✅ Makindo Exam Pearls
- Zone 3 is most vulnerable to hypoxia and paracetamol toxicity.
- INR is an early marker of reduced hepatic synthesis; albumin reflects chronic reserve.
- Paracetamol overdose: conjugation saturates → ↑ NAPQI → glutathione depletion → centrilobular necrosis; NAC restores glutathione.
- First-pass metabolism and reduced albumin explain why “standard doses” can be too strong in decompensated cirrhosis.
📌 Conclusion
The liver’s structure (segments, sinusoids, zonation) is inseparable from its function (metabolism, synthesis, bile, detox). Drug handling depends on blood flow, CYP activity, conjugation capacity, and biliary transport - all of which change in liver disease. Paracetamol toxicity neatly demonstrates these principles: Phase II saturation plus Zone 3 CYP metabolism creates NAPQI, and glutathione depletion drives predictable hepatocyte injury.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery