
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anthrax (Bacillus anthracis)
⚠️ Early diagnosis of Anthrax and the prompt initiation of combination antimicrobial therapy are critical for survival. 💨 Inhalational anthrax, in particular, carries a high mortality if untreated and requires immediate critical care involvement.
📖 About
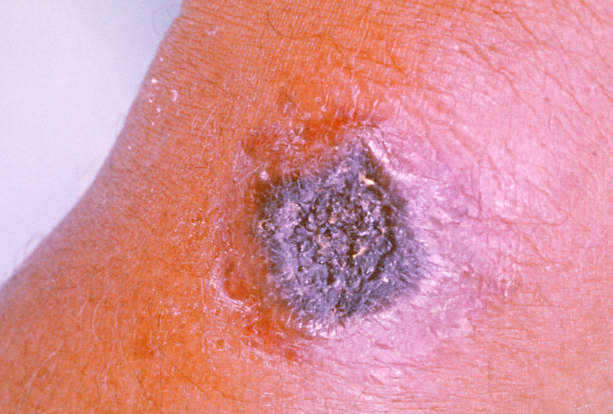
- 🐏 Anthrax (from Greek “coal”) refers to the black eschar in cutaneous disease.
- Caused by Bacillus anthracis, a spore-forming zoonotic bacterium that infects herbivores.
- Transmission occurs via contaminated hides, wool, or meat; also relevant in bioterrorism.
🔬 Characteristics
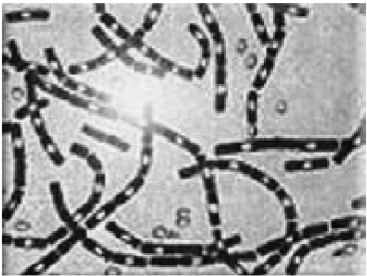
- Gram-positive, aerobic, spore-forming bacillus.
- 🌱 Spores can persist in soil/environment for decades.
- 🛡️ Polypeptide capsule (D-glutamic acid) is antiphagocytic.
- Infection routes: skin, inhalation, ingestion → systemic disease possible.
Eschars

🌍 Source
- Contaminated soil, carcasses, and animal products (hides, wool, meat).
- Endemic in:
- 🌎 Central & South America
- 🌍 Sub-Saharan Africa
- 🌏 Asia & Eastern Europe
- 🌴 The Caribbean
- 🔺 Bioterrorism example: US anthrax letters (2001).
🧪 Virulence
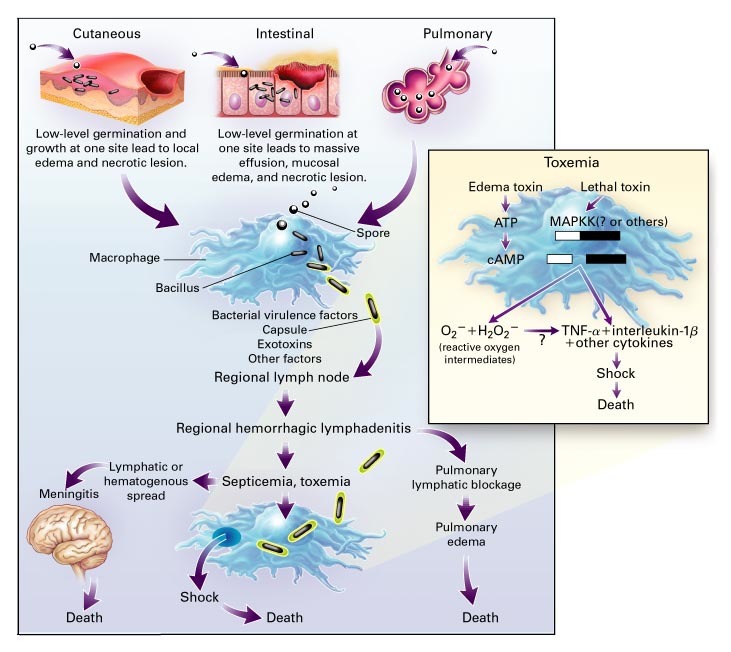
- 🛡️ Protective antigen (PA): enables toxin entry into host cells.
- ☠️ Lethal factor (LF): cleaves MAP kinase → apoptosis.
- 💧 Oedema factor (EF): ↑cAMP → fluid leak & immune dysregulation.
- Combined → necrosis, oedema, haemorrhage, immune evasion.
🧠 Pathophysiology
🤒 Clinical Forms
- 🖐️ Cutaneous Anthrax (~95% cases):
- Entry via skin abrasions → painless ulcer + black eschar.
- Can progress to lymphadenitis & systemic infection.
- 💨 Inhalational Anthrax (“wool sorters’ disease”):
- Flu-like prodrome → rapid respiratory distress, cyanosis, shock.
- Classic sign: widened mediastinum ± pleural effusion.
- Mortality >50% untreated.
- 🍖 Gastrointestinal Anthrax:
- From undercooked infected meat.
- Nausea, bloody diarrhoea, perforation, high mortality.
- 🩸 Systemic Anthrax:
- Shock, renal failure, DIC, meningitis (often haemorrhagic & fatal).
🔍 Investigations
- 🔬 Microscopy: Gram stain, special staining (e.g., Ziehl-Neelsen variant).
- 🧪 McFadyen’s reaction: polychrome methylene blue → capsule seen.
- 🧬 PCR & Culture: confirmatory, though culture may be slow.
- 📷 CXR: widened mediastinum, pleural effusions in inhalational form.
- 🧪 Bloods & serology: capsular antigen detection.
💊 Management (Infectious Diseases input essential)
- 🛡️ Prevention: vaccination in military/veterinary at-risk groups.
- 🚑 Supportive: ABC resuscitation, oxygen, IV fluids, ITU if severe.
- 💊 Antibiotics:
- First-line: Ciprofloxacin, Levofloxacin, or Doxycycline.
- Combination therapy (e.g., add aminoglycoside/rifampin).
- If susceptible: Benzyl Penicillin may be used (esp. cutaneous).
- ❌ Avoid cephalosporins (resistance).
- 🧴 Antitoxins: Raxibacumab (monoclonal antibody) or anthrax immunoglobulin for systemic disease.
- 💉 Prophylaxis: 60 days of ciprofloxacin or doxycycline after spore exposure.
- ➕ Corticosteroids (e.g., dexamethasone) for meningitis or airway oedema.
💊 Anthrax – Typical Antimicrobial Dosing (verify with BNF/datasheet)
| Scenario | Drug & Dose |
|---|---|
| 🖐️ Cutaneous Anthrax (mild, non-systemic) |
Ciprofloxacin 500 mg PO BD (7–10 days)
OR
Doxycycline 100 mg PO BD (7–10 days)
💡 If systemic features → use IV + combination therapy. |
| 💨 Inhalational Anthrax / Systemic infection |
Ciprofloxacin 400 mg IV every 12h
OR
Doxycycline 100 mg IV every 12h
➕ Add 1–2 additional agents (rifampicin, clindamycin, or aminoglycoside) for synergy. Duration: ≥60 days (due to persistent spores). |
| 🧠 Anthrax meningitis (suspected/confirmed) | Ciprofloxacin IV (as above) ➕ Rifampicin IV ➕ Clindamycin IV (Triple therapy recommended). |
| 🧴 Post-exposure prophylaxis (PEP) |
Ciprofloxacin 500 mg PO BD for 60 days
OR
Doxycycline 100 mg PO BD for 60 days.
➕ Anthrax vaccine where available. |

📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery