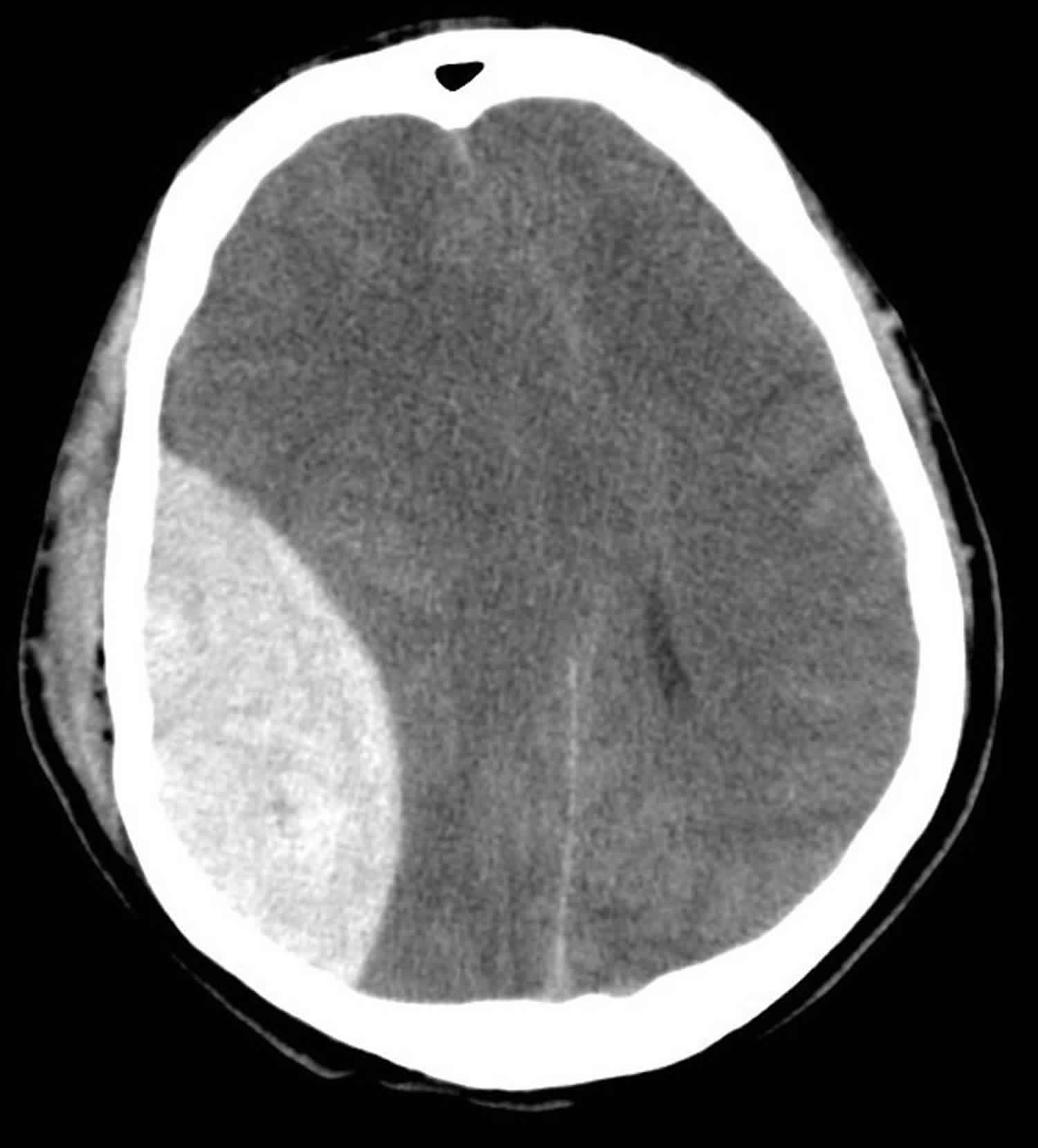
Epidural Haematoma
Related Subjects:
|
Brain Herniation syndromes
|
Epidural Haematoma
|
Subdural haematoma
|
Extradural haematoma
🧠 Epidural haemorrhage (EDH) often follows blunt head trauma with a skull fracture and can evolve rapidly.
A lucid interval (initial recovery then deterioration) is a classic clue but is not always present.
⚠️ Treat EDH as a time-critical neurosurgical emergency: deterioration can reflect rising ICP and impending herniation.
📖 Overview
- Epidural haemorrhage (EDH) (also “extradural haematoma”) is bleeding between the dura mater and the inner table of the skull.
- Most are arterial, classically from the middle meningeal artery after a temporal/parietal skull fracture.
- Expanding EDH → mass effect → raised ICP → risk of uncal/central herniation and secondary brain injury.
- More common in young people (dura less adherent); mechanism often high-energy trauma (RTA, fall, assault, sports).
🩸 Aetiology & Risk Factors
- Trauma is the usual cause: skull fracture lacerating the middle meningeal artery or branches (often temporoparietal).
- Skull fracture is common (often quoted ~70–95%), but EDH can occur without a visible fracture.
- Venous EDH (dural sinus/diploic veins) occurs less often; consider with vertex/posterior fossa location, or in children/older adults.
- Rare non-traumatic contributors: coagulopathy/anticoagulation, vascular lesions, infection eroding bone (uncommon).
🔬 Pathophysiology
- Bleeding dissects dura away from skull → biconvex (lentiform) collection.
- Typically does not cross suture lines (dural attachments at sutures limit spread).
- Arterial EDH can enlarge quickly → compression, midline shift, and herniation syndromes.
- Posterior fossa EDH is uncommon but dangerous: small volumes can cause rapid brainstem compression and obstructive hydrocephalus.
🩺 Clinical Features
- Pattern: head injury → (possible brief LOC) → possible lucid interval → worsening headache, vomiting, confusion, falling GCS.
- Focal deficits: contralateral weakness, aphasia (dominant hemisphere), seizures.
- Herniation red flags: ipsilateral fixed dilated pupil (CN III), progressive bradycardia/hypertension (Cushing response), irregular respirations.
- Don’t be reassured by early “well appearance” - EDH can be a “talk and deteriorate” lesion.
🧪 Investigations
- Non-contrast CT head is first-line and time-critical: look for biconvex hyperdensity, mass effect, midline shift, and associated fracture.
- Swirl sign (hypodense area within clot) suggests active bleeding and higher risk of expansion.
- Use bone windows to assess fracture; consider CT venography if vertex EDH/sinus injury suspected.
- Repeat CT/urgent re-scan if neurological status changes, even if the initial scan was “small EDH”.
⚡ Management
- ABCDE first (simultaneous escalation): protect C-spine, optimise oxygenation and ventilation, maintain perfusion and avoid hypotension/hypoxia.
- Early neurosurgical involvement - EDH is a neurosurgical emergency. In the UK, involve the regional neurosurgical centre early and document advice.
- Reverse coagulopathy urgently where relevant (e.g., PCC + vitamin K for warfarin; specific DOAC reversal per local guideline; platelets/DDAVP only in selected contexts).
- Bridge measures for raised ICP while arranging transfer/theatre: head-up 30°, analgesia/sedation, maintain normocapnia; hypertonic saline/mannitol per protocol; brief hyperventilation only if impending herniation and as a temporising step.
- Typical surgical triggers (always defer to neurosurgery/local protocol): large volume, significant thickness, midline shift, deterioration in GCS, focal deficit/anisocoria, posterior fossa EDH, or features suggesting ongoing bleed.
- Small EDH with stable neurology may be managed conservatively with HDU/ICU neuro-observations and planned repeat imaging.
🧠 Teaching pearl (pathophysiology): EDH is dangerous because arterial bleeding can expand quickly in a confined space. As ICP rises, cerebral perfusion pressure falls (CPP = MAP − ICP), risking secondary ischaemic injury even before herniation. The classic “lucid interval” reflects temporary compensation before decompensation - but many patients never show it, so the safe rule is to treat deterioration after head injury as EDH (or other intracranial bleed) until proven otherwise.
📌 Differentials to keep in mind
- Subdural haematoma: crescentic, can cross sutures, often from bridging veins; may be acute or chronic.
- Traumatic SAH and contusions: may coexist; symptoms can overlap.
- Diffuse axonal injury: disproportionate coma with minimal CT findings early.
📚 Key References & Further Reading
