Related Subjects:
|Causes of abnormal Vaginal bleeding
|Vaginal Carcinoma
|Cervical cancer
|Endometrial (Uterine) Cancer
|Post Menopausal Bleeding
|AP of the Uterus and Fallopian Tubes
|AP of the Ovary
|Gynaecological History Taking
|Colposcopy
|Premature Menopause
|Polycystic Ovary syndrome
ℹ️ About
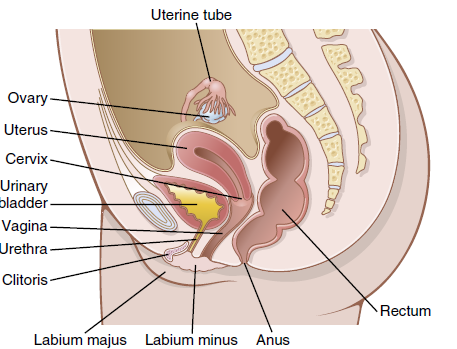
- The uterus is a hollow, thick-walled muscular organ situated in the true pelvis between the bladder anteriorly and rectum posteriorly.
- It communicates superiorly with the fallopian (uterine) tubes and inferiorly with the vagina via the cervix.
- Its primary roles are menstruation, implantation, fetal development, and parturition.
- It is composed of three distinct layers: perimetrium (outer), myometrium (middle), and endometrium (inner).
🔬 Uterus – Gross Anatomy
- Parts: Fundus (above tubal openings), body, isthmus, and cervix.
- Position: Normally anteverted and anteflexed (tilted forward over the bladder).
- Size (non-pregnant): ~7–8 cm long, 5 cm wide, ~40 g in weight.
🧱 Layers of the Uterine Wall
- Perimetrium: Outer serosal layer (visceral peritoneum).
- Myometrium: Thick smooth muscle layer arranged in:
- Outer longitudinal fibres (merge with supporting ligaments)
- Middle circular/spiral fibres (rich vascular supply; key for haemostasis postpartum)
- Inner longitudinal/oblique fibres
- Endometrium: Inner mucosal layer with:
- Functional layer (shed during menstruation)
- Basal layer (regenerates functional layer)
🔄 Physiology of the Uterus
- Menstrual cycle: Oestrogen stimulates proliferative growth; progesterone induces secretory transformation.
- Implantation: Occurs in the secretory phase when endometrium is thick, vascular, and glandular.
- Labour: Coordinated myometrial contractions mediated by oxytocin and prostaglandins.
- Postpartum: Spiral muscle fibres constrict uterine vessels, reducing haemorrhage.
🤰 Changes in Pregnancy
- Weight increases from ~40 g to ~1 kg at term.
- Growth occurs primarily via hypertrophy of existing smooth muscle cells (rather than hyperplasia).
- Oestrogen promotes myometrial growth; progesterone maintains uterine quiescence.
- Stretching and hormonal effects increase uterine blood flow dramatically.
🩸 Blood Supply
- Primarily from the uterine arteries (branches of the internal iliac arteries).
- Additional supply from ovarian arteries (branches of the abdominal aorta).
- Uterine artery runs in the base of the broad ligament and crosses over the ureter (“water under the bridge”).
- Extensive anastomosis supports pregnancy and protects against ischaemia.
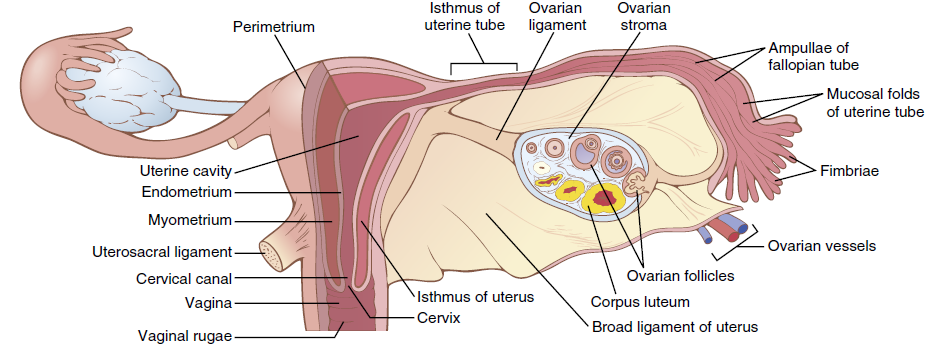
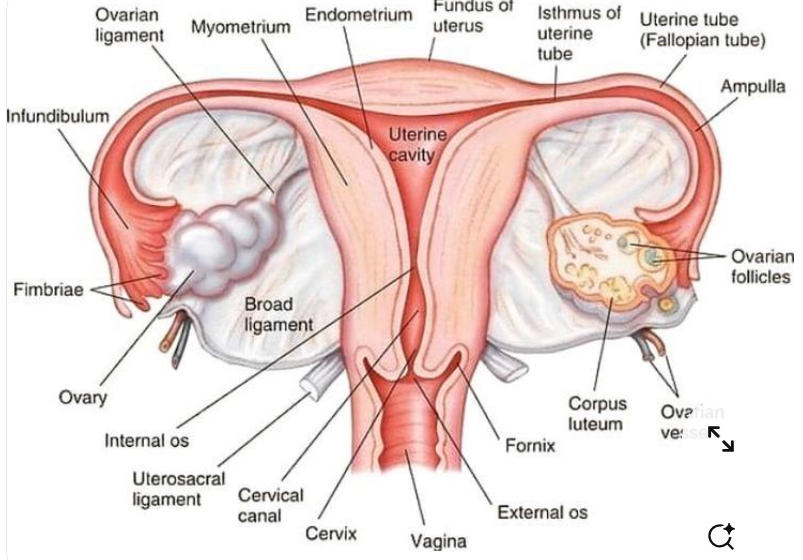
🧵 Cervix
- Cylindrical lower portion of the uterus (~2–3 cm long).
- Internal os (to uterine cavity) and external os (to vagina).
- Rich in collagen and connective tissue with limited smooth muscle.
- Softens in late pregnancy due to prostaglandins and collagen remodelling.
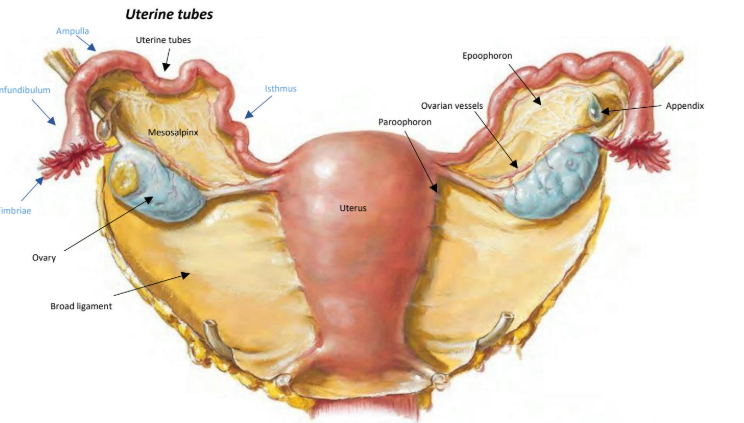
🌸 Fallopian (Uterine) Tubes – Anatomy
- Paired muscular tubes ~10–12 cm long.
- Extend from uterine cornua to the ovaries.
- Four parts:
- Infundibulum: Funnel-shaped end with fimbriae.
- Ampulla: Widest part; usual site of fertilisation.
- Isthmus: Narrow medial segment.
- Intramural (interstitial): Passes through uterine wall.
⚙️ Fallopian Tube Physiology
- Oocyte capture: Fimbriae sweep ovulated oocyte into tube.
- Fertilisation: Usually occurs in the ampulla.
- Transport: Coordinated ciliary beating and smooth muscle peristalsis move embryo toward uterus.
- Hormonal regulation: Oestrogen enhances ciliary activity; progesterone slows transport.
🩺 Clinical Correlations
- Ectopic pregnancy most commonly occurs in the ampulla.
- Pelvic inflammatory disease can damage cilia → infertility.
- Uterine fibroids arise from the myometrium.
- Cervical incompetence may cause mid-trimester loss.
