
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Metabolic acidosis
Related Subjects: |Metabolic acidosis |Aspirin or Salicylates toxicity |Ethylene glycol toxicity |Renal Tubular Acidosis |Lactic acidosis |Metabolic alkalosis
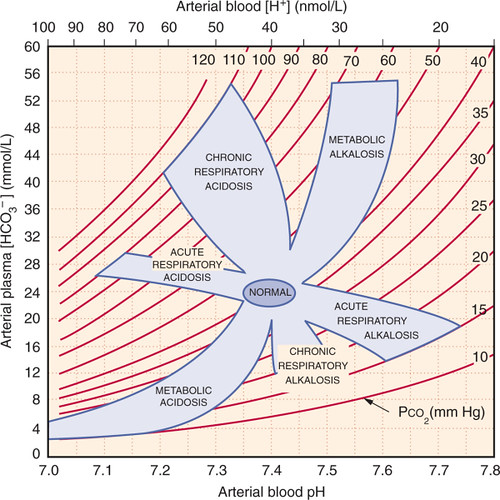
🧪 Analysis of Metabolic Acidosis (ABG)
- pH < 7.35 (unless compensated).
- HCO₃⁻ < 22 mmol/L.
- PaCO₂ usually low (<5.3 kPa) due to respiratory compensation (hyperventilation).
- PaO₂ often normal.
- Base Excess < -2.
⚡ Aetiology
- Accumulation of organic or inorganic acids.
- Loss of bicarbonate (HCO₃⁻).
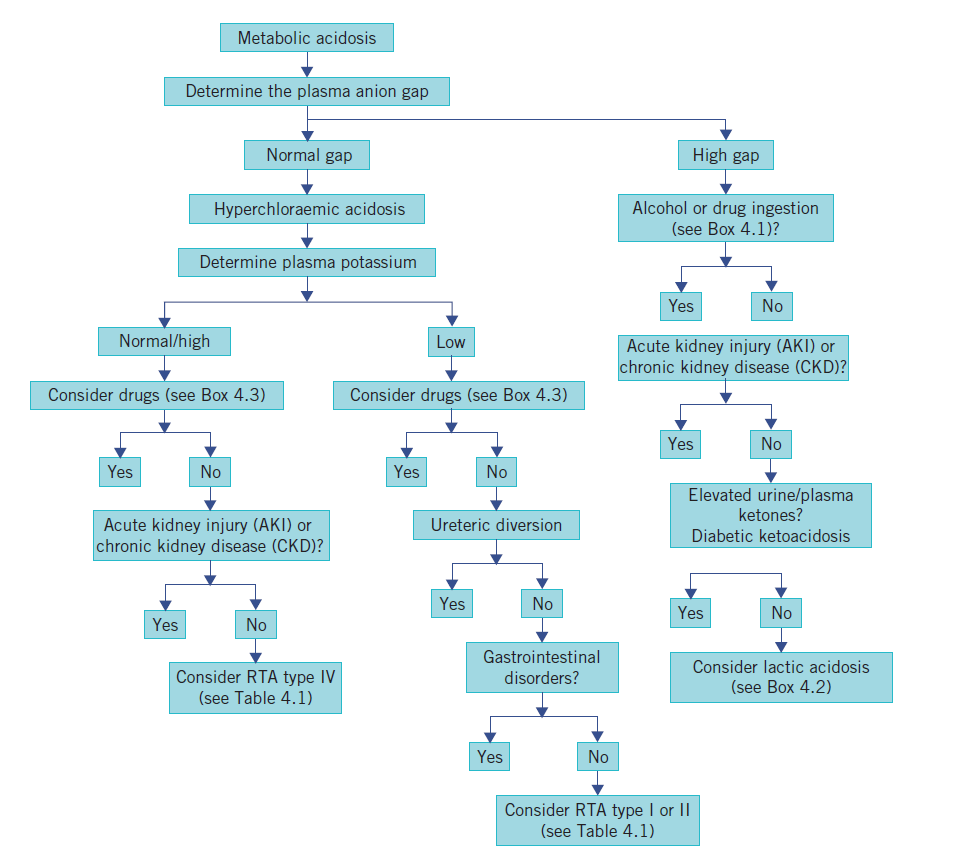
- Anion Gap (AG) = (Na⁺ + K⁺) – (Cl⁻ + HCO₃⁻). Normal = 8–12 mmol/L.
📊 Causes by Anion Gap
| 🔺 High Anion Gap | ➡️ Normal Anion Gap |
|---|---|
|
|
🧠 Clinical Features
- Hyperventilation (Kussmaul breathing).
- Underlying cause often obvious (shock, DKA, diarrhoea etc.).
- AG helps narrow differential.
🔎 Key Anion Gap Markers
| Anion | Clinical Case |
|---|---|
| 🧪 L-Lactate | Anaerobic metabolism (shock, sepsis). |
| 🍩 Beta-hydroxybutyrate | Diabetic ketoacidosis. |
| 🧴 Hippurate | Toluene poisoning (glue sniffers). |
| 🥛 Glycolate & Oxalate | Methanol/ethylene glycol ingestion. |
| 🌿 D-Lactate | Gut fermentation (e.g., blind loop syndrome). |
💊 Management by Cause
| Cause | Clinical Features | Diagnostic Tests | Management |
|---|---|---|---|
| 💉 Lactic Acidosis | Shock, sepsis, hypoxia, confusion, tachypnoea. | ABG (low pH/HCO₃⁻), serum lactate ↑. | Oxygen, IV fluids, treat cause, inotropes (noradrenaline if septic shock). |
| 🍩 Ketoacidosis | Polyuria, polydipsia, fruity breath, dehydration, confusion. | ABG (low pH, low HCO₃⁻), ketones ↑, glucose ↑ (DKA). | IV fluids, insulin infusion (if DKA), K⁺ replacement, monitor glucose & ketones. |
| 🩺 Renal Failure | Oedema, oliguria, confusion, uremia. | Creatinine ↑, urea ↑, ABG acidosis, electrolytes (hyperkalaemia). | Dialysis if severe, correct underlying cause, treat K⁺ imbalance. |
| ☠️ Toxins | Visual loss (methanol), renal failure (ethylene glycol), tinnitus (salicylates). | ABG: HAGMA, osmolar gap ↑, toxin assays. | Fomepizole, dialysis, bicarbonate (salicylates). |
| 💩 Diarrhoea | Loose stools, dehydration, cramps, lethargy. | ABG: NAGMA, low K⁺, low Na⁺. | Rehydrate (oral/IV), replace electrolytes, treat cause (infection, malabsorption). |
| ⚡ Renal Tubular Acidosis | Polyuria, weakness, bone pain, growth delay (children). | ABG: NAGMA, urine pH pattern, electrolytes. | Oral bicarbonate (NaHCO₃ or K-citrate), treat cause. |
| 🧂 Hyperchloremic Acidosis | Weakness, confusion, oedema if fluid overload. | ABG: NAGMA, Cl⁻ ↑, HCO₃⁻ ↓. | Stop saline infusion, use balanced fluids (Hartmann’s/Ringer’s), correct electrolytes. |
🩺 Case 1 - Diabetic Ketoacidosis (DKA)
A 24-year-old woman with type 1 diabetes presents with abdominal pain, vomiting, and drowsiness. Vitals: HR 120, BP 95/60, RR 28 with Kussmaul breathing. Labs: glucose 28 mmol/L, ketones 6 mmol/L, pH 7.15, HCO₃⁻ 10 mmol/L. Management: 💉 Fixed-rate IV insulin infusion, IV fluids (0.9% saline initially), potassium replacement as guided, identify trigger (infection). Avoid: ❌ Bicarbonate therapy unless pH <6.9; avoid rapid fluid shifts in young patients (risk of cerebral oedema).
🩺 Case 2 - Lactic Acidosis in Sepsis
A 68-year-old man presents with fever, hypotension, and confusion. BP 80/50, HR 120, lactate 6.2 mmol/L, pH 7.22, HCO₃⁻ 14 mmol/L. Diagnosis: septic shock with lactic acidosis. Management: 🚑 Sepsis 6 bundle - IV fluids, broad-spectrum antibiotics, oxygen, source control. Consider vasopressors if hypotension persists. Avoid: ❌ Delaying antibiotics; avoid excessive normal saline (can worsen acidosis with hyperchloraemia).
🩺 Case 3 - Renal Failure (Uraemic Acidosis)
A 75-year-old woman with stage 5 chronic kidney disease presents with progressive weakness, nausea, and confusion. Labs: pH 7.28, HCO₃⁻ 16 mmol/L, high urea and creatinine, potassium 6.0 mmol/L. Management: 🩺 Sodium bicarbonate therapy if symptomatic and not fluid overloaded, treat hyperkalaemia, dialysis if severe or refractory. Avoid: ❌ Relying on IV fluids alone; avoid potassium-sparing drugs (e.g. spironolactone, ACEI) in the acute setting.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery