
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Diabetes: Eye Disease
Related Subjects: |Diabetes Mellitus: Basics |Type 1 Diabetes Mellitus | Type 2 Diabetes Mellitus | Type 3c Diabetes Mellitus |Insulin Physiology |Gestational Diabetes |HbA1c |Hyperglycaemic Hyperosmolar State (HHS) |Diabetic Nephropathy |Diabetic Retinopathy |Diabetic Neuropathy |Diabetic Amyotrophy |Maturity Onset Diabetes of the Young (MODY) |Diabetes: Complications |Hypoglycaemia |Diabetic Ketoacidosis (DKA) Adults |Alcoholic Ketoacidosis |Euglycaemic Ketoacidosis (euDKA) with SGLT2 Inhibitors |Causes of Ketoacidosis |Gold Score: Hypoglycaemia Awareness in Type 1 Diabetes
👁️ Diabetic retinopathy is largely preventable: tight glycaemic control, BP and lipids slow microvascular damage; timely laser/anti-VEGF preserves sight. In the UK, routine annual screening from age 12 (NHS DES) catches asymptomatic disease early.
📖 About
- ~50% of T1D affected within 10–15 years; ~50% of T2D within 15 years. Most changes are mild if detected early.
- Risk rises with diabetes duration, hyperglycaemia (HbA1c), hypertension, dyslipidaemia, nephropathy, pregnancy, and smoking.
🧠 Pathophysiology (why VEGF rises)
- Chronic hyperglycaemia → pericyte loss, basement-membrane thickening, capillary dropout → retinal ischaemia.
- Ischaemia ↑VEGF → ↑permeability (macular oedema) and fragile neovascularisation (proliferative disease).
🩺 Screening (UK focus)
- Annual mydriatic digital photography (NHS DES). Symptomless until late stages-screening is crucial.
- Pregnancy (pre-existing diabetes): retinal assessment at booking (1st trimester) and again at 28 weeks; if retinopathy at booking, add a review at 16–20 weeks.
🔎 Classification → what it means
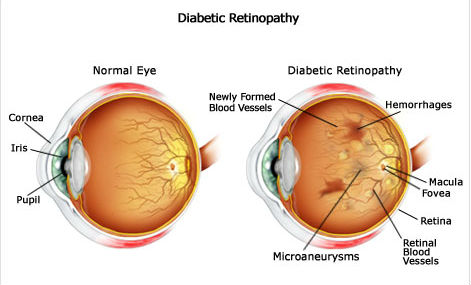
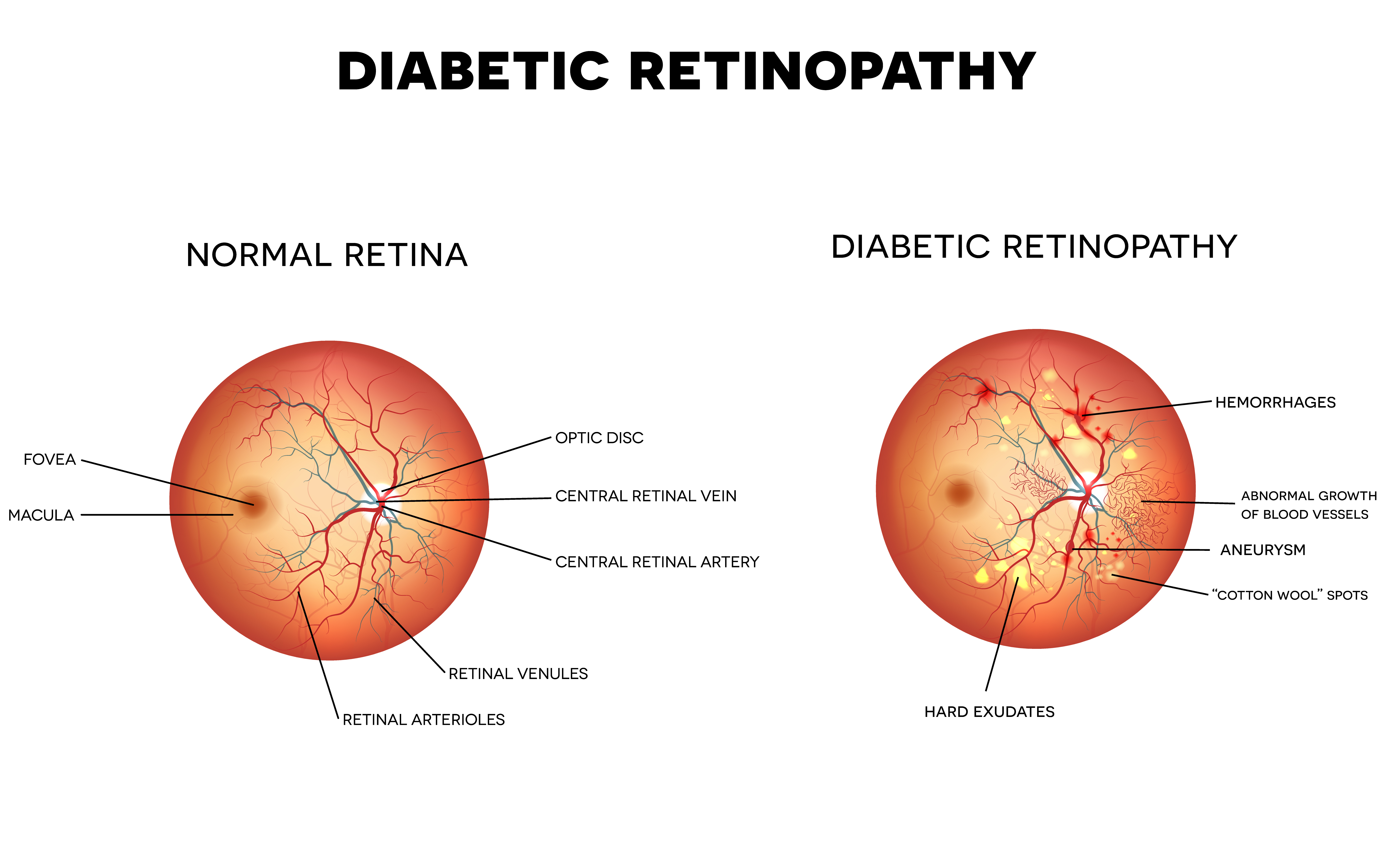
- Background (R1): microaneurysms, dot/blot haemorrhages, hard exudates. Usually asymptomatic.
- Pre-proliferative (R2): venous beading, multiple blot haemorrhages, IRMA/cotton-wool spots = significant ischaemia.
- Proliferative (R3): new vessels at disc/elsewhere ± pre-retinal/vitreous haemorrhage → high risk of tractional detachment.
- Maculopathy (M1): macular oedema/exudates within 1 disc diameter of fovea or reduced acuity from oedema.
🚦Referral urgency (practical)
- 🔴 R3 or M1 with reduced vision: urgent same-week ophthalmology (often same-day if vitreous haemorrhage/sudden floaters or vision drop).
- 🟠 R2: prompt routine referral (weeks).
- 🟢 R1: continue annual screening; optimise risk factors.
🧰 Management
- Risk factor optimisation: individualised HbA1c target, strict BP control, statin/ACEi as indicated, smoking cessation.
- Macular oedema (centre-involving): intravitreal anti-VEGF (e.g., aflibercept/ranibizumab); steroids in selected cases.
- Proliferative retinopathy: pan-retinal photocoagulation (PRP); anti-VEGF as adjunct/bridge.
- Advanced disease: vitrectomy for non-clearing vitreous haemorrhage or tractional retinal detachment.
⚠️ Red flags (act now)
- Sudden floaters, curtain over vision, or acute vision drop → possible vitreous haemorrhage/retinal detachment → same-day eye assessment.
- Pregnancy with progressive retinopathy → expedite ophthalmology review.
📚 Teaching diagram placeholders
🧑⚕️ Case vignette
A 58-year-old with T2D (12 yrs), HbA1c 74 mmol/mol, BP 154/92, reports mild central blur. Screening photo shows hard exudates within 1DD of the fovea and thickening on OCT. ✅ M1 maculopathy → refer urgently for anti-VEGF; tighten BP and glucose; start/optimise statin and ACEi.
💡 Mentor tip
If you remember just three things for viva: duration drives risk, VEGF links ischaemia to oedema/neovascularisation, and R3/M1 need urgent eyes-on. Everything else is risk-factor medicine.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery