Related Subjects:
|Brain tumour s
|Astrocytomas
|Brain Metastases
|Tuberous sclerosis
|Turcot's syndrome
|Lhermitte Duclos Disease
|Oligodendroglioma
|Acute Hydrocephalus
|Intracranial Hypertension
|Primary CNS Lymphoma (PCNSL)
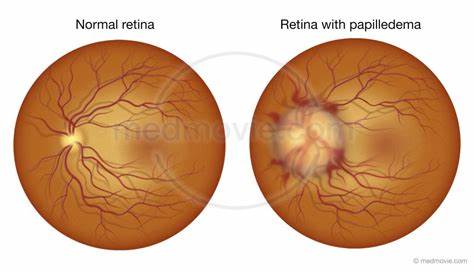
👁️ Papilloedema is swelling of the optic disc due to raised intracranial pressure (ICP).
It requires emergency referral to ophthalmology/neuro services and urgent brain imaging (including MRV/CTV to exclude cerebral venous sinus thrombosis).
The mechanism of optic nerve damage is axoplasmic flow stasis causing intraneuronal ischaemia → untreated cases risk permanent vision loss.
📍 About
- Represents venous outflow obstruction, inflammation, or raised ICP.
- Optic disc swelling due to impaired axoplasmic transport.
- May occur with raised CSF pressure, intracranial mass, or systemic causes.
⚠️ Causes
- Raised ICP:
- Brain tumours (supra- and infratentorial).
- Abscess, oedema.
- Haemorrhage (ICH, SAH, SDH, EDH).
- Encephalitis, hydrocephalus.
- Cerebral venous sinus thrombosis (CVT).
- Sarcoidosis, Guillain–Barré (↑ CSF protein).
- Idiopathic intracranial hypertension (IIH).
- Malignant hypertension.
- Retro-orbital lesions (e.g. cavernous sinus thrombosis).
- Optic neuritis / uveitis (inflammatory).
- Ischaemia (e.g. accelerated HTN).
- CO₂ retention.
🔎 Pseudopapilloedema
- Optic disc drusen or congenital disc anomalies.
- Disc infiltration (inflammatory or neoplastic).
- Down syndrome (associated anomalies).
Assessing optic discs can be challenging. Mydriasis is not usually required, but 0.5% tropicamide can be used if necessary.
Always document if dilating drops are used.
🩺 Clinical Features
- Visual acuity often preserved until late - but document carefully.
- Early sign = loss of spontaneous venous pulsation.
- Optic disc looks swollen/oedematous, with blurred margins.
- Grey/blurred vision, transient visual obscurations, diplopia.
- Fundoscopy: hyperaemia, flame haemorrhages, cotton-wool spots.
- Visual field loss (enlarged blind spot, peripheral constriction).
- Systemic: headache, nausea, vomiting, pulsatile tinnitus.
🧠 Differentials
- Pseudopapilloedema (disc drusen, anomalies).
- Optic neuritis (painful, ↓ acuity early, RAPD present).
- Anterior ischaemic optic neuropathy.
🔬 Investigations
- CT/MRI + venogram (CTV/MRV): First step → rule out mass lesion & venous thrombosis.
- If imaging excludes mass lesion → LP with opening pressure for ICP assessment.
💊 Management
- Hypertension: Aggressive BP control in malignant HTN.
- Mass lesion: Urgent referral to neurosurgery.
- CVT: Anticoagulate + neurology input.
- IIH: Weight reduction, acetazolamide, neuro-ophthalmology review, regular visual field monitoring.
- Other optic nerve/eye disease: Ophthalmology referral.
📌 Exam Tip
Papilloedema = raised ICP until proven otherwise.
👉 Always do neuroimaging before lumbar puncture to avoid coning.
Fundoscopy: swollen disc, blurred margins, venous engorgement, haemorrhages.
Vision preserved early - differentiates from optic neuritis.
📚 References
