Acute Disc Prolapse
Related Subjects:
|Transverse myelitis
|Acute Disseminated Encephalomyelitis
|Cervical spondylosis
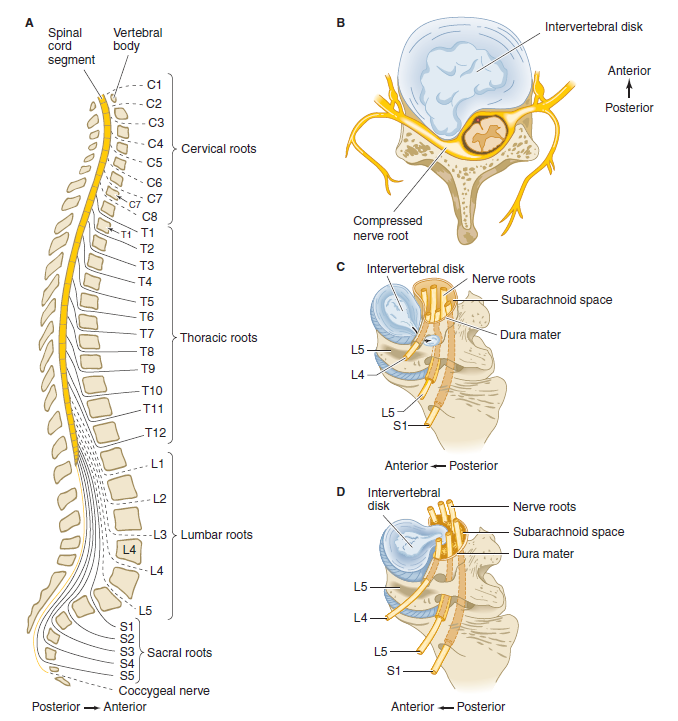
|Spinal Cord Anatomy
|Acute Disc Prolapse
|Spinal Cord Compression
|Spinal Cord Haematoma
|Foix-Alajouanine syndrome
|Cauda Equina
|Conus Medullaris syndrome
|Anterior Spinal Cord syndrome
|Central Spinal Cord syndrome
|Brown-Sequard Spinal Cord syndrome
|Internal Decapitation
🧾 About
- Acute Disc Disease: 💥 Often presents with partial spinal cord symptoms, particularly in older adults following trauma (e.g., a fall).
- Central disc herniation can compress the cauda equina (LMN signs 🦵), while lateral herniations usually impact specific nerve roots.
- Disc prolapse is more common in younger individuals due to higher water content in discs, but degeneration with age increases risk in older patients.
🧬 Aetiology
- The disc herniates backward through a tear in the annulus fibrosus, with the nucleus pulposus protruding into the spinal canal.
- This can compress:
- Spinal cord → producing UMN signs (spasticity, brisk reflexes, Babinski).
- Cauda equina → producing LMN signs (flaccid paralysis, areflexia, saddle anaesthesia).
- Nerve root → leading to radiculopathy with focal weakness, numbness, and dermatomal pain.
⚠️ Causes
- Acute trauma (falls, heavy lifting, twisting injuries).
- Chronic degeneration from age-related disc dehydration and narrowing of intervertebral spaces.
- Repetitive strain or poor lifting techniques in manual labour.
🩺 Clinical Presentation
- Sudden, severe lumbar back pain often after a specific movement (e.g., bending, coughing, sneezing).
- Protective muscle spasm causing a tilted posture or reduced mobility.
- Pain typically radiates down the leg (sciatica) and worsens with movement. Most commonly involves L4/5 or L5/S1 discs.
- Central lesions → risk of cauda equina syndrome (urinary retention, saddle anaesthesia, bilateral leg weakness 🚨).
- Lateral lesions → radicular pain and weakness in a dermatomal/myotomal pattern.
🧪 Neurological Findings by Nerve Root
- S1: Pain buttock → calf → sole of foot, sensory loss in sole/calf, weak plantar flexion, absent ankle jerk.
- L5: Pain buttock → lateral leg → dorsum of foot, weak dorsiflexion (foot drop), ↓ straight-leg raise.
- L4: Pain lateral thigh → medial calf, sensory loss calf, ↓ knee reflex, positive femoral stretch test.
🔍 Investigations
- Blood tests: FBC, U&E, ESR/CRP, ALP, phosphate, calcium → exclude infection/malignancy.
- MRI spine: Gold standard for confirming disc prolapse, nerve root compression, or cauda equina features.
- CT spine: Alternative if MRI is contraindicated, though less sensitive for soft tissue lesions.
💊 Management
- Conservative: Analgesia (NSAIDs, opioids if severe), firm mattress, stay active (bed rest discouraged).
- Physiotherapy: Once pain settles → restore mobility, improve core strength, correct posture.
- Corticosteroid injections: Can reduce inflammation in persistent radicular pain.
- Surgical referral 🚨: Urgent if red flag symptoms (bladder dysfunction, saddle anaesthesia, progressive motor weakness) → possible decompression/discectomy.
