
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Adrenal Gland
Related Subjects: |AP of the Thyroid |AP of the Parathyroid |AP of the Pituitary |AP of the Pancreas |AP of the Adrenal Gland |Addisons Disease |Phaeochromocytoma |Adrenal Adenomas |Adrenal Cancer |Cushing Syndrome |Cushing Disease |Congenital Adrenal hyperplasia |Primary hyperaldosteronism (Conn's syndrome) |ACTH |McCune Albright syndrome
🧠 The adrenal glands are paired endocrine organs that cap the superomedial poles of the kidneys. They coordinate the body’s response to stress and maintain blood pressure, sodium–water balance, glucose availability, and immune modulation. Each adrenal gland contains two functionally distinct tissues: the adrenal cortex (steroid hormones) and the adrenal medulla (catecholamines). Clinically, adrenal disease often presents with changes in blood pressure, electrolytes, weight, pigmentation, or episodic “adrenergic” symptoms.
📍 1) Gross Anatomy and Relations
- Location: Retroperitoneal, on the superior pole of each kidney within renal fascia and perirenal fat (but separate from the kidney by a thin septum).
- Shape:
- Right adrenal: pyramidal; lies close to the IVC and posterior to the liver.
- Left adrenal: crescent/semilunar; related to stomach, spleen, pancreas tail, and left kidney.
- Hilum: Medial aspect where vessels and nerves enter/exit (especially the single adrenal vein).
📌 Clinical: Adrenals have a very rich arterial supply but a single main vein on each side, which matters in surgery and in venous sampling.
🩸 2) Blood Supply, Venous Drainage, and Lymphatics
- Arterial supply (three sources):
- Superior suprarenal arteries (from inferior phrenic artery)
- Middle suprarenal artery (from abdominal aorta)
- Inferior suprarenal arteries (from renal artery)
- Venous drainage (single main vein):
- Right suprarenal vein → IVC (short, fragile)
- Left suprarenal vein → left renal vein (often receives inferior phrenic vein)
- Lymph: Para-aortic (lumbar) nodes.
🧬 3) Embryology and Tissue Identity
- Adrenal cortex: derived from mesoderm (coelomic epithelium).
- Adrenal medulla: derived from neural crest (chromaffin cells = modified post-ganglionic sympathetic neurons).
This dual origin explains why the cortex behaves like a classic steroid endocrine gland, while the medulla is essentially a specialised sympathetic organ that releases catecholamines straight into blood.
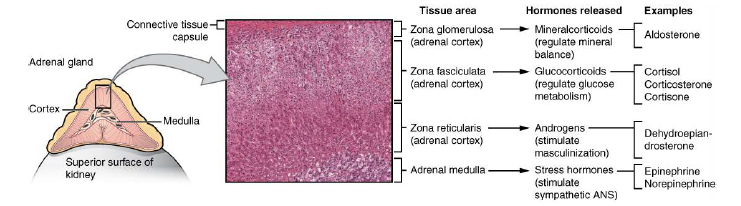
🏗️ 4) Microscopic Anatomy: Cortex Zones and Medulla
🟤 Adrenal Cortex (outer) - “GFR” from outside in
- Zona Glomerulosa (outermost) → Mineralocorticoids (mainly aldosterone)
- Zona Fasciculata (middle, largest) → Glucocorticoids (mainly cortisol)
- Zona Reticularis (inner) → Androgens (mainly DHEA, androstenedione)
⚡ Adrenal Medulla (inner)
- Chromaffin cells produce catecholamines: adrenaline (epinephrine) and noradrenaline (norepinephrine).
- Surrounded by fenestrated capillaries for rapid hormone release.
🧠 Key integration: Cortisol from the cortex bathes the medulla via local blood flow and upregulates PNMT (phenylethanolamine-N-methyltransferase), the enzyme that converts noradrenaline → adrenaline. So the cortex helps “tune” medullary output.
🧪 5) Steroidogenesis: What the Cortex Makes and From What
All adrenal cortical hormones are made from cholesterol. Steroid hormones are lipid-soluble and synthesized on demand (not stored in vesicles). A core early step is cholesterol transport into mitochondria by StAR (steroidogenic acute regulatory protein) and conversion to pregnenolone.
- Zona glomerulosa: lacks 17α-hydroxylase → specialises in aldosterone synthesis.
- Zona fasciculata: uses 17α-hydroxylase → makes cortisol.
- Zona reticularis: shifts toward androgen precursors (DHEA).
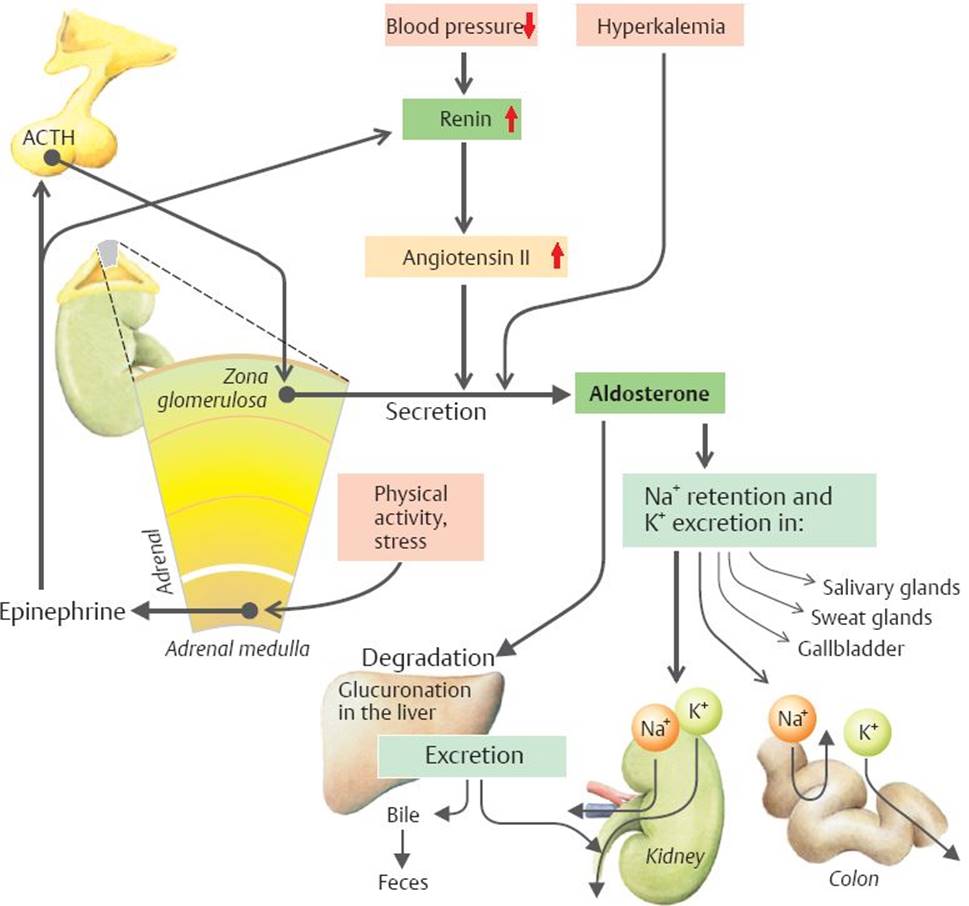
🧂 6) Aldosterone: Physiology and Regulation (Zona Glomerulosa)
- Main job: maintain effective circulating volume and potassium balance.
- Target: distal nephron (late distal tubule/collecting duct principal cells).
- Actions:
- ↑ ENaC and Na⁺/K⁺-ATPase → ↑ Na⁺ reabsorption (water follows) → ↑ BP/volume
- ↑ K⁺ secretion → risk of hypokalaemia when excessive
- ↑ H⁺ secretion (α-intercalated cells) → can contribute to metabolic alkalosis
🎛 Regulation of Aldosterone
- RAAS (dominant): ↓ renal perfusion / ↓ NaCl at macula densa → renin → angiotensin II → ↑ aldosterone.
- Plasma potassium: ↑ K⁺ directly stimulates aldosterone release (protects against hyperkalaemia).
- ACTH: minor transient stimulation only (not the main controller).
📌 Clinical pattern: Excess aldosterone → hypertension + hypokalaemia + metabolic alkalosis (not always hypokalaemic).
🍬 7) Cortisol: Physiology, Circadian Rhythm, and Stress (Zona Fasciculata)
- Main job: ensure adequate fuel supply and maintain vascular responsiveness during stress.
- Metabolic effects: ↑ gluconeogenesis, ↑ lipolysis, ↑ proteolysis → ↑ blood glucose; contributes to insulin resistance.
- Immune effects: anti-inflammatory and immunosuppressive (↓ cytokines, ↓ eosinophils, redistribution of leukocytes).
- Cardiovascular: permissive for catecholamines → maintains vascular tone and BP.
- Bone/skin: chronic excess → osteoporosis, skin thinning, bruising, striae.
- Secretion pattern: pulsatile with diurnal rhythm (peak early morning; nadir around midnight) and rises with acute stress.
🎛 Regulation (HPA axis)
- Hypothalamus: CRH (± AVP) →
- Pituitary: ACTH →
- Adrenal cortex: cortisol → negative feedback on CRH/ACTH
📌 Clinical: Exogenous steroids suppress ACTH → adrenal atrophy; abrupt withdrawal can precipitate adrenal crisis. Always taper long courses.
⚧️ 8) Adrenal Androgens (Zona Reticularis)
- Main products: DHEA, DHEA-S, androstenedione (weak androgens; peripheral conversion to testosterone/oestrogens).
- Physiological role: contributes to pubic/axillary hair and libido (especially in females); minor contribution to male androgen status (testes dominate).
- Regulation: largely ACTH-driven.
⚡ 9) Adrenal Medulla: Catecholamines and “Fight-or-Flight”
The adrenal medulla is a specialised sympathetic organ. Preganglionic sympathetic fibres (ACh) stimulate chromaffin cells to release catecholamines into the bloodstream, creating a rapid whole-body stress response.
- Hormones: adrenaline (often predominant) and noradrenaline.
- Triggers: pain, hypoglycaemia, haemorrhage, fear, exercise, hypoxia.
- Key effects (receptor-mediated):
- β1: ↑ heart rate and contractility → ↑ cardiac output
- β2: bronchodilation; vasodilation in skeletal muscle; ↑ glycogenolysis
- α1: vasoconstriction → ↑ BP; mydriasis
- Metabolic: ↑ glucose availability (glycogenolysis/gluconeogenesis), ↑ lipolysis
🧠 High-yield link: Cortisol upregulates PNMT in the medulla → promotes adrenaline production.
🩺 10) Clinical Syndromes (Patterns You Recognise at the Bedside)
⬇️ Primary Adrenal Insufficiency (Addison’s disease)
- Mechanism: loss of adrenal cortex → low cortisol ± low aldosterone.
- Typical features: fatigue, weight loss, postural hypotension, abdominal pain, salt craving.
- Key labs: hyponatraemia, hyperkalaemia, hypoglycaemia; ↑ ACTH in primary disease.
- Hyperpigmentation: due to high ACTH/POMC derivatives (only in primary, not secondary).
- Emergency: adrenal crisis → shock, vomiting, severe hypotension; treat with IV hydrocortisone + fluids.
⬆️ Cushing’s syndrome (excess cortisol)
- Causes: exogenous steroids (commonest), pituitary ACTH adenoma (Cushing disease), ectopic ACTH, adrenal tumour.
- Features: central weight gain, proximal myopathy, thin skin/bruising, striae, hypertension, glucose intolerance, infections, osteoporosis, mood changes.
🧂 Primary hyperaldosteronism (Conn syndrome)
- Causes: adrenal adenoma or bilateral hyperplasia.
- Pattern: hypertension + suppressed renin; ± hypokalaemia; metabolic alkalosis.
- Symptoms: weakness/cramps (low K⁺), polyuria/polydipsia.
⚡ Phaeochromocytoma
- Origin: chromaffin cells (adrenal medulla) or extra-adrenal paraganglioma.
- Classic symptoms: episodic headache, palpitations, sweating, tremor, panic; paroxysmal or sustained hypertension.
- Key management principle: α-blockade before β-blockade (to avoid unopposed α vasoconstriction).
🧪 11) Practical Testing Overview (Quick UK-Style Orientation)
- Suspected adrenal insufficiency: 9am cortisol ± short synacthen test; check renin/aldosterone if primary suspected.
- Suspected Cushing’s: screening with overnight dexamethasone suppression, late-night salivary cortisol, or 24h urinary free cortisol (then source localisation).
- Suspected hyperaldosteronism: aldosterone–renin ratio (ARR) then confirmatory testing and imaging/venous sampling when indicated.
- Suspected phaeochromocytoma: plasma metanephrines or urinary metanephrines, then imaging.
📊 Quick Revision Table
| Region | Main Hormone(s) | Main Trigger | Headline Effect |
|---|---|---|---|
| Zona glomerulosa | Aldosterone | Ang II, ↑K⁺ | ↑ Na⁺ retention, ↑ BP; ↑ K⁺/H⁺ excretion |
| Zona fasciculata | Cortisol | ACTH (CRH) | Stress adaptation, ↑ glucose, anti-inflammatory, maintains vascular tone |
| Zona reticularis | DHEA/androgens | ACTH | Pubarche/libido (esp. females), androgen precursors |
| Medulla | Adrenaline/NA | Sympathetic ACh | Fight-or-flight: ↑ HR/BP, bronchodilation, ↑ glucose |
📝 Summary
The adrenal gland is two endocrine systems in one: the cortex (steroids: aldosterone, cortisol, androgens) and the medulla (catecholamines). Aldosterone is RAAS/K⁺-driven and defends volume and potassium; cortisol is ACTH-driven and coordinates metabolic and immune responses to stress; adrenal androgens support pubertal hair and libido; catecholamines deliver rapid sympathetic “fight-or-flight” physiology. Recognising pattern presentations (Addison’s, Cushing’s, Conn syndrome, phaeochromocytoma) is high-yield because the physiology explains the bedside findings.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery