
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Larynx
Related Subjects:
|Anatomy of the Ear
|AP of the Oesophagus
|AP of the Diaphragm
|AP of the Large Bowel (Colon, Rectum, Anal Canal)
|AP of Small Bowel
|AP of the Biliary system
|AP of the Bone Marrow
|Anatomy of the Eye
|AP of the Larynx
|Anatomy of the Ear
|Anatomy of the Ear
|Anatomy of the Pharynx
|Anatomy of the Nose
|Anatomy of Male Genitalia
|Anatomy of Breast
|Anatomy of the Stomach
|Anatomy of the Rectum
|Anatomy of the Spleen
🎤 The larynx (“voice box”) is a highly specialised organ in the anterior neck, spanning roughly C3–C6.
It sits between the pharynx and trachea and functions as:
It achieves these functions through a cartilaginous framework, intricate intrinsic muscles, and precise sensory–motor innervation via the vagus nerve.
📍 Position, Relations & Surface Landmarks
- Location: anterior neck, suspended from the hyoid, continuous inferiorly with the trachea.
- Anterior relations: strap muscles (infrahyoids) and thyroid gland (especially anterior/lateral to lower larynx).
- Posterior relations: laryngopharynx; oesophagus begins posteriorly at cricopharyngeus level.
- Key palpable landmarks:
- Thyroid cartilage (“Adam’s apple”).
- Cricothyroid membrane between thyroid and cricoid cartilages (front-of-neck access).
- Cricoid cartilage (firm complete ring).
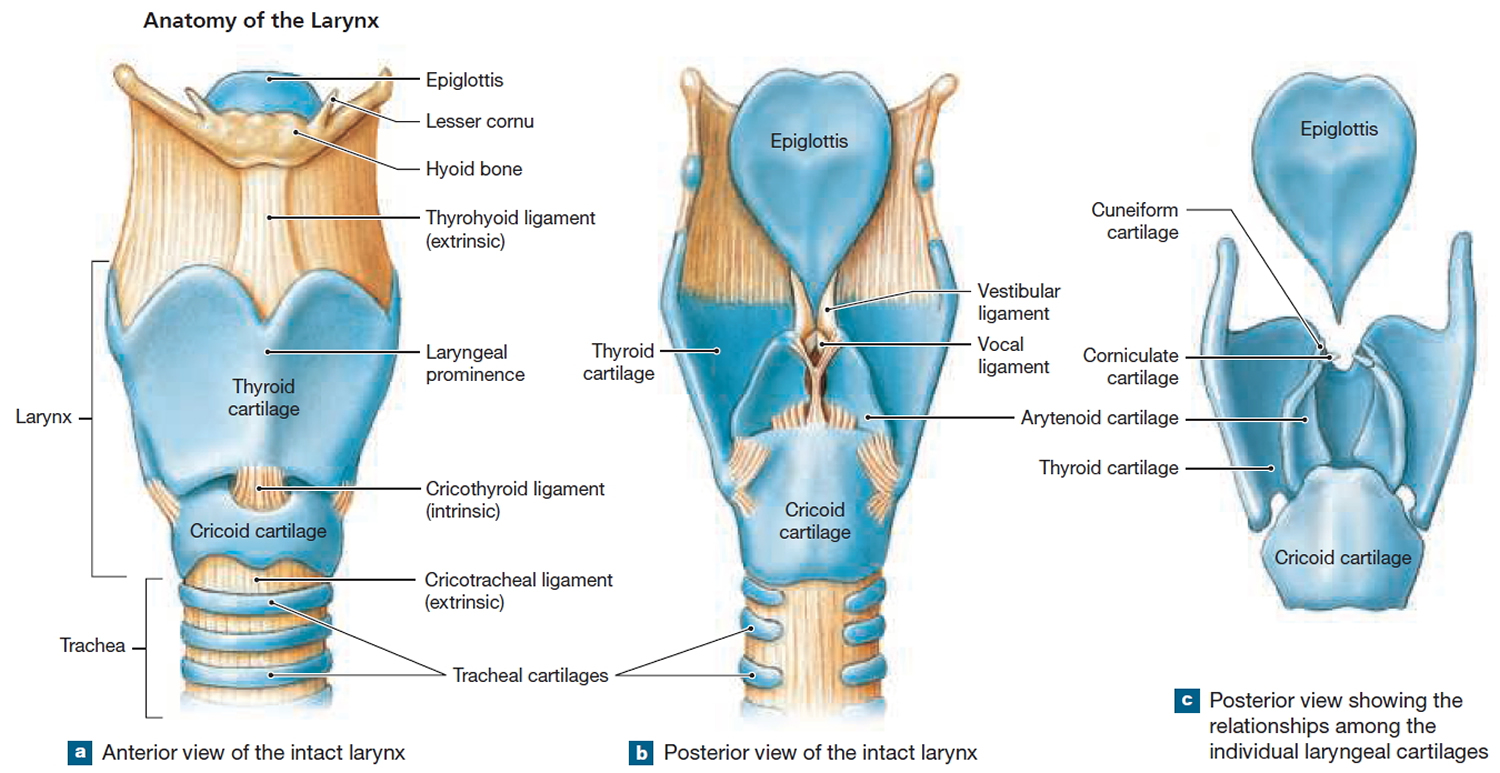
🧱 Cartilaginous Framework
The laryngeal cartilages form a protective “box” with mobile joints that allow fine adjustment of vocal fold position and tension. The cricoid is the only complete ring; the arytenoids are the key moving parts that abduct/adduct the vocal folds.
- Unpaired cartilages
- Thyroid cartilage: largest; forms the anterior wall and protects the vocal folds.
📌 Clinical: landmark for laryngeal level and emergency airway orientation. - Cricoid cartilage: complete ring; forms the base of the larynx; articulates with thyroid (cricothyroid joints) and arytenoids (cricoarytenoid joints).
📌 Exam tip: functionally crucial in airway patency; paediatric airway is narrow and easily compromised. - Epiglottis: leaf-shaped elastic cartilage; folds posteriorly during swallowing to help protect the laryngeal inlet.
- Thyroid cartilage: largest; forms the anterior wall and protects the vocal folds.
- Paired cartilages
- Arytenoids: sit on cricoid lamina; rotate/slide to abduct/adduct vocal folds and adjust tension.
- Corniculates: small “horns” on arytenoids; support posterior laryngeal inlet.
- Cuneiforms: support aryepiglottic folds and maintain inlet patency.
🪢 Ligaments, Membranes & Joints
- Extrinsic supports
- Thyrohyoid membrane: suspends larynx from hyoid; transmits the internal branch of SLN and superior laryngeal vessels.
- Cricotracheal ligament: connects cricoid to trachea.
- Intrinsic fibroelastic membranes
- Quadrangular membrane: forms the vestibular (false) fold margin superiorly; contributes to supraglottic structure.
- Cricovocal membrane (conus elasticus): forms the vocal ligament margin inferiorly; essential for true vocal folds.
- Cricothyroid membrane (median part): high-yield emergency access site (front-of-neck airway).
- Key synovial joints
- Cricothyroid joints: tilt thyroid cartilage forward/back → changes vocal fold tension (pitch control).
- Cricoarytenoid joints: arytenoid rotation/glide → vocal fold abduction/adduction (airway vs phonation).
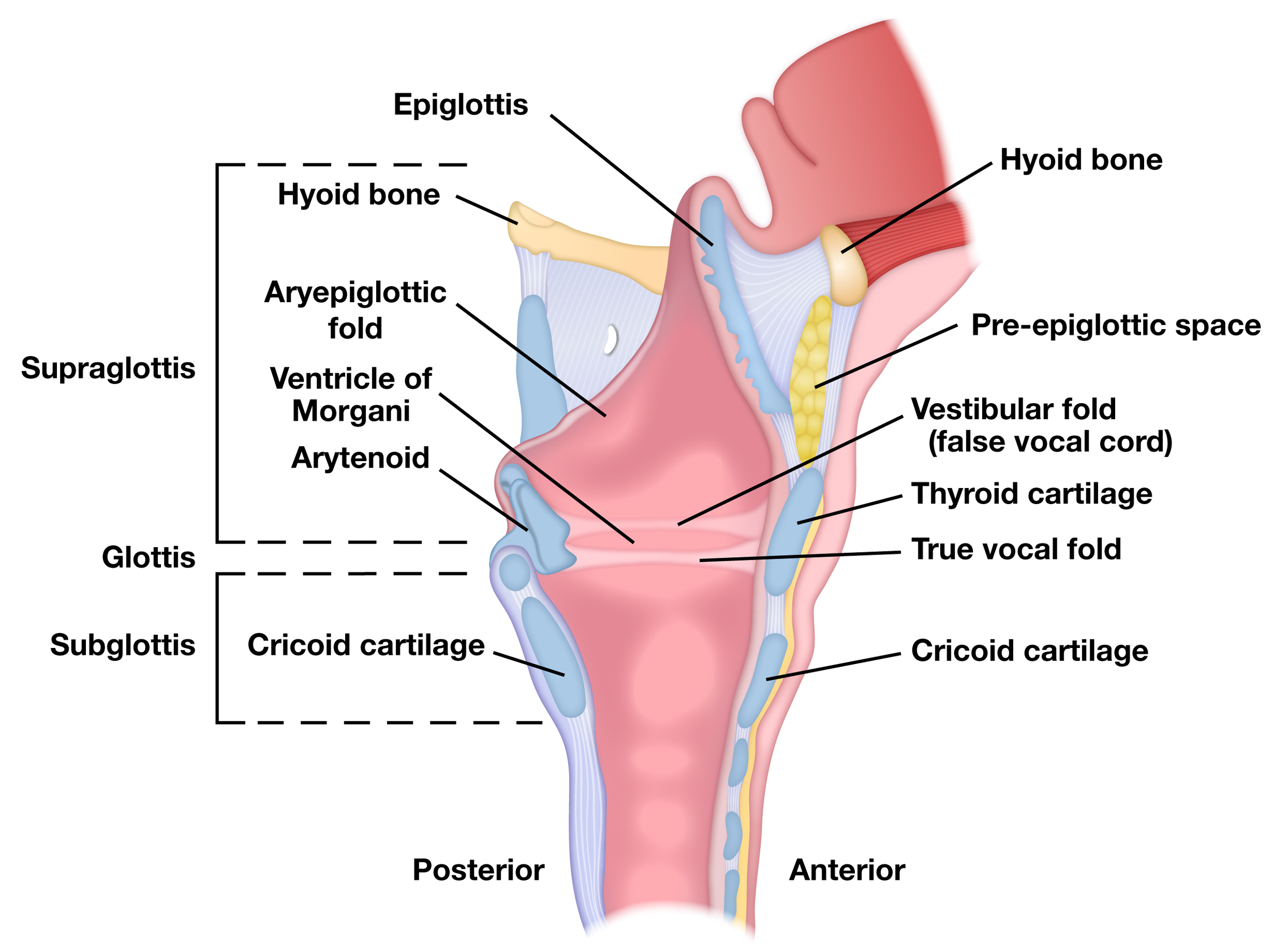
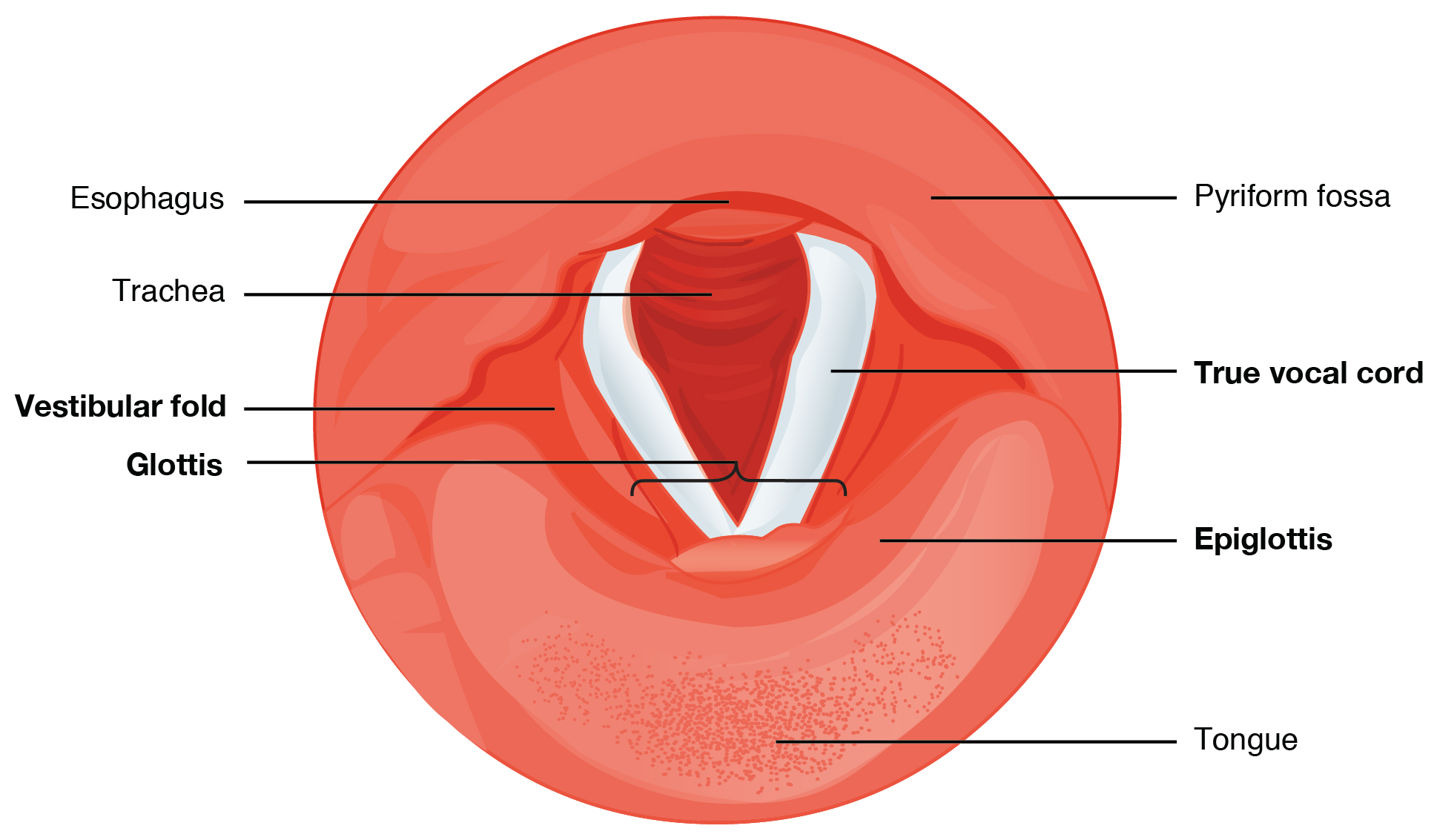
🏛️ Internal Divisions of the Laryngeal Cavity
- Supraglottis: epiglottis, aryepiglottic folds, vestibule, and false (vestibular) folds.
🛡️ Main role: airway protection and shaping airflow. - Glottis: true vocal folds + rima glottidis (the opening between them).
🎶 Main role: phonation; also critical for airway resistance and cough. - Subglottis: from below the vocal folds to inferior cricoid border → trachea.
📌 Important in paediatric airway obstruction and subglottic stenosis.
🎶 True vs False Cords (What’s the difference?)
- False (vestibular) folds: protective, contribute to resonance and closure during swallowing/straining; not the main sound source.
- True vocal folds: contain the vocal ligament + vocalis muscle; vibrate to create sound.
- Covered by stratified squamous epithelium to withstand friction.
- The superficial lamina propria (“Reinke’s space”) is important for normal vibration and is affected in Reinke’s oedema.
💪 Musculature
Intrinsic laryngeal muscles provide fine control of vocal fold position and tension (airway vs voice). Extrinsic muscles move the whole larynx up/down, crucial during swallowing and speech.
- Intrinsic muscles (key actions)
- Posterior cricoarytenoid: only abductor → opens rima glottidis (breathing).
📌 Bilateral dysfunction → potentially life-threatening airway compromise (stridor). - Lateral cricoarytenoid: adducts vocal folds (phonation, airway protection).
- Interarytenoids (transverse/oblique): adduct arytenoids → closes posterior glottis.
- Cricothyroid: tenses/elongates vocal folds → ↑ pitch (🎵).
Nerve: external branch of superior laryngeal nerve. - Thyroarytenoid + vocalis: fine-tune tension and mass → controls timbre, pitch modulation, and subtle voice quality.
- Posterior cricoarytenoid: only abductor → opens rima glottidis (breathing).
- Extrinsic muscles (move larynx as a unit)
- Suprahyoids elevate larynx during swallowing.
- Infrahyoids (strap muscles) depress/stabilise larynx during speech and after swallowing.
🩸 Blood Supply & Lymphatics
- Arteries:
- Superior laryngeal artery (from superior thyroid artery).
- Inferior laryngeal artery (from inferior thyroid artery).
- Veins: drain via superior/inferior thyroid veins.
- Lymphatics: classically divided by the vocal folds:
- Supraglottis: rich lymphatics → upper deep cervical nodes.
- Glottis: relatively sparse lymphatics → early cancers may present with hoarseness before nodal spread.
- Subglottis: drains to pretracheal/paratracheal and lower deep cervical nodes.
🧠 Innervation (High-yield)
The larynx is innervated by the vagus nerve (CN X) via the superior laryngeal nerve and recurrent laryngeal nerve. A simple rule: RLN does almost all motor, except cricothyroid (external SLN). Sensation is split by vocal fold level.
- Superior laryngeal nerve (SLN)
- Internal branch: sensation to supraglottis (above vocal folds); triggers protective cough reflex when stimulated.
- External branch: motor to cricothyroid (pitch control).
- Recurrent laryngeal nerve (RLN)
- Motor to all other intrinsic laryngeal muscles (abduction/adduction/closure).
- Sensory to subglottis (below vocal folds).
- 📌 Clinical: unilateral palsy → hoarseness/weak voice; bilateral palsy → airway obstruction/stridor.
⚙️ Physiology
🌬️ 1) Respiration and Airway Resistance
- The larynx regulates airflow by altering rima glottidis size.
- Abduction of vocal folds during inspiration reduces resistance; slight narrowing can increase airflow velocity (useful in certain speech sounds).
- Protective reflexes (cough, laryngospasm) prevent aspiration but can acutely obstruct airflow.
🎶 2) Phonation (Sound Production)
Voice is produced when air from the lungs passes through adducted vocal folds, causing them to vibrate. Pitch depends largely on vocal fold tension/length (cricothyroid + vocalis control), while loudness depends on subglottic pressure and degree of closure. The supraglottic tract (pharynx, oral/nasal cavities) shapes resonance to create intelligible speech.
- Adduction (lateral cricoarytenoid + interarytenoids) approximates cords for vibration.
- Tension control:
- Cricothyroid: increases tension/length → ↑ pitch.
- Vocalis: fine-tunes stiffness and segmental vibration → nuanced tone.
- Resonance/articulation: shaped by pharynx, tongue, palate, lips (larynx is the sound source; upper airway is the “instrument body”).
🛡️ 3) Swallowing & Airway Protection
- Laryngeal elevation (suprahyoids) moves larynx upward/anteriorly, helping open the upper oesophageal sphincter and protecting the airway.
- Epiglottic deflection plus aryepiglottic fold closure helps shield the inlet.
- Vocal fold closure (true cords) and vestibular fold approximation provide a layered seal.
- Reflexes: supraglottic sensory input (internal SLN) triggers cough/laryngospasm if material approaches the inlet.
💥 4) Pressure Functions (Valsalva, Cough, Lifting)
- Glottic closure enables generation of high intrathoracic pressure for:
- Cough (airway clearance)
- Valsalva manoeuvre (straining)
- Stabilisation during lifting
⚕️ Clinical Relevance
- 🗣️ Vocal cord paralysis: RLN injury (thyroid/parathyroid surgery, mediastinal/lung pathology) → hoarseness, aspiration, weak cough; bilateral palsy can cause stridor.
- 🎵 External SLN injury: weak/monotone voice, impaired high pitch/projection (cricothyroid dysfunction) - important in professional voice users.
- 🛠️ Airway procedures: cricothyrotomy uses the cricothyroid membrane; intubation requires knowledge of glottic anatomy to avoid trauma.
- 🤧 Laryngitis: inflammation → hoarseness; persistent hoarseness needs assessment.
- 🧪 Laryngeal cancer: persistent hoarseness (especially >3 weeks), dysphagia/odynophagia, neck lumps → urgent ENT pathway.
- 🧒 Paediatric airway: small calibre means oedema causes large resistance increase → croup/subglottic narrowing can be dramatic.
📌 Key Exam Pearls
- Posterior cricoarytenoid = only vocal fold abductor.
- RLN supplies all intrinsic muscles except cricothyroid (external SLN).
- Sensation: above cords = internal SLN; below cords = RLN.
- Glottis is the primary sound source; supraglottis is crucial for protection and resonance shaping.
✅ Conclusion
The larynx is a finely balanced organ integrating respiration, phonation, and airway protection. Its cartilages provide a stable yet mobile framework; intrinsic muscles precisely position and tense the vocal folds; and vagal innervation partitions sensation and motor control in a clinically predictable pattern. Understanding these anatomy–physiology links underpins safe airway management, thyroid/neck surgery, and early recognition of laryngeal pathology.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery