
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
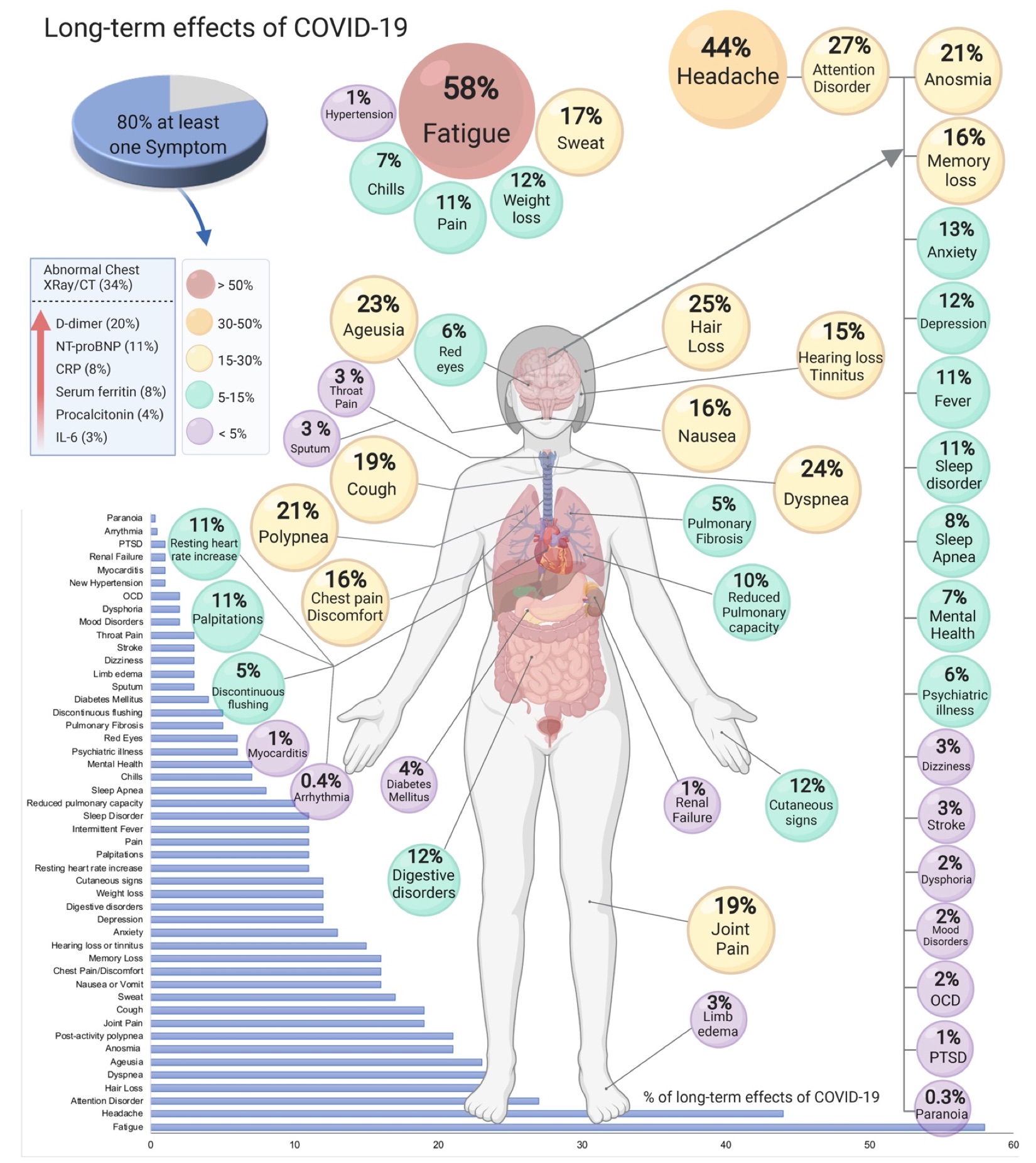
Long COVID
🧠 Long COVID (Post-COVID-19 condition) - persistent or new symptoms ≥12 weeks after acute infection, not explained by an alternative diagnosis. Multisystem; fluctuating course; pacing and symptom-guided rehab are central.
🗂️ One-Page Clinical Summary (no extra CSS)
| Domain | Common features | Initial approach (primary care) |
|---|---|---|
| Energy / Fatigue | Profound fatigue; post-exertional symptom exacerbation (PESE/PEM); unrefreshing sleep | 🧭 Teach pacing & energy envelope; avoid fixed graded exercise. Sleep hygiene; screen for anaemia, thyroid, B12, ferritin, HbA1c; occupational/education adjustments. |
| Breathlessness / Chest | Dyspnoea, chest tightness, cough; palpitations | Vitals incl. SpO₂; CXR (≥12 wks if persistent), ECG; consider BNP if HF symptoms; inhaler trial if variable wheeze/cough. Safety-net for red flags. |
| Neurocognitive | “Brain fog”, poor concentration, headaches, dizziness | Rule out depression, anxiety, sleep apnoea, migraine. Cognitive pacing, task chunking, screen/limit multitasking; consider work/study accommodations. |
| Autonomic / Orthostatic | Orthostatic intolerance, tachycardia (possible PoTS), temperature dysregulation | Active stand test; fluids 2–3 L/day, ↑salt if appropriate, compression stockings, slow position changes. Consider propranolol/ivabradine under specialist advice if PoTS suspected. |
| MSK / Pain | Myalgia, arthralgia, deconditioning | Gentle flexibility and symptom-contingent strengthening within energy envelope; heat/ice; simple analgesia; avoid NSAIDs if gastritis risk. |
| Mental health | Anxiety, low mood, PTSD-like symptoms | Validate; brief CBT-informed strategies; peer support; consider SSRIs/SNRIs if indicated; manage insomnia. |
| GI | Nausea, diarrhoea, abdominal pain | Hydration; low-FODMAP trial if IBS-like (short term, dietitian if possible); rule out red flags; treat reflux/IBS per guidelines. |
| ENT / Olfactory | Hyposmia/anosmia, dysgeusia | Olfactory training (twice daily, 12+ weeks); treat rhinitis/reflux if present. |
🧪 Baseline Assessment (rule out differentials)
| Tests | Why | Notes |
|---|---|---|
| FBC, U&E, LFTs, CRP, ferritin, TSH, HbA1c, B12/folate | Screen for anaemia, thyroid disease, inflammation, diabetes, deficiencies | Target correctables that mimic fatigue/brain fog |
| ECG; consider CXR (persistent respiratory symptoms ≥12 wks) | Exclude occult cardiopulmonary disease | Troponin/BNP guided by symptoms/exam |
| Urinalysis; pulse oximetry (rest/exertional) | Renal screen; exertional desaturation | 6-minute walk if safe; stop if symptomatic |
| Directed tests | Only if red flags (PE, myocarditis, new neuro deficits) | D-dimer/CTPA, echo, neuro imaging per presentation |
🛡️ Red Flags (urgent same-day assessment)
- New/worsening chest pain, syncope, resting SpO₂ <94% (or <92% in COPD) or exertional desaturation
- Focal neurology, severe new headache, confusion
- Haemoptysis, calf swelling/pleuritic pain (consider PE)
- Cardiac red flags after COVID (myocarditis/pericarditis features)
🎯 Management & Follow-up
- Education & pacing: plan-do-review diary; avoid “boom-bust”.
- Rehab: breathing control, gentle mobility, then symptom-contingent strengthening; refer to local Long COVID / pulmonary rehab services when available.
- Sleep: regular schedule, light exposure, limit naps/caffeine; consider melatonin short-term.
- Autonomic care: fluids/salt, compression, recumbent exercise start; meds via specialist if PoTS.
- Return to work/school: phased, with adjustments; provide fit note specifying limitations.
- Vaccination: associated with lower risk of developing Long COVID; keep up to date.
🧑🏫 Patient-friendly message
“Long COVID can wax and wane. Working within your energy limits, prioritising sleep, and tackling one problem at a time usually helps. We’ll rule out other causes, support your rehab, and review regularly. Seek urgent help if you develop chest pain, fainting, or new breathlessness.”
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery