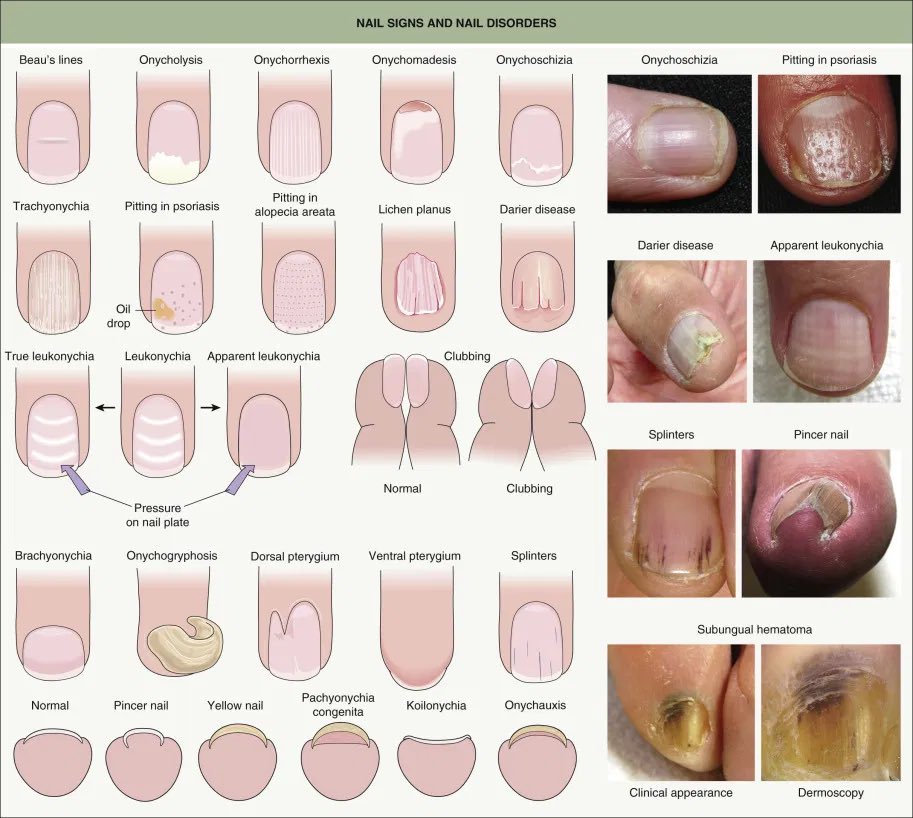
| 🧩 Psoriasis |
Pitting, onycholysis, oil-drop/salmon patch, subungual hyperkeratosis |
Cutaneous plaques, scalp disease, PsA symptoms; consider topical steroid or calcipotriol |
| 🌀 Alopecia areata |
Regular geometric pitting, trachyonychia, longitudinal ridging |
Patchy non-scarring hair loss, atopy; topical/intralesional steroid if needed |
| 📏 Lichen planus |
Longitudinal ridging, thinning, dorsal pterygium, fissuring |
Violaceous pruritic papules, oral lacy lesions; refer to derm (risk of scarring) |
| 🍄 Onychomycosis |
Yellow-brown discoloration, distal-lateral onycholysis, subungual debris |
Tinea pedis, occlusive footwear, diabetes; confirm mycology before oral antifungal therapy |
| 🫁 Clubbing |
Spongy nail bed, loss of Schamroth window, Lovibond angle >180° |
Lung disease (Ca, bronchiectasis, IPF), IBD, cyanotic heart disease, cirrhosis; investigate underlying cause |
| 🥄 Koilonychia |
“Spoon” nails (concave) |
Iron deficiency anaemia (FBC/ferritin), congenital forms; treat underlying cause |
| 📉 Beau’s lines |
Transverse depressions |
Systemic illness, chemotherapy, severe infection; nails normalise as they grow |
| 🩸 Splinter haemorrhages |
Longitudinal reddish-brown streaks |
Trauma most common; consider infective endocarditis if fever, murmur, emboli |
| 🤍 Terry’s nails |
Proximal 80% white, distal rim pink |
Cirrhosis, heart failure, diabetes, ageing; assess liver/cardiac status |
| 🌓 Lindsay’s nails |
Proximal white, distal brown ~20–60% |
Chronic kidney disease; review renal function |
| 📐 Onycholysis |
Distal nail plate separation |
Psoriasis, thyrotoxicosis, trauma, tetracyclines; keep nail short/dry |
| 🦠 Paronychia (acute) |
Periungual erythema, pain, pus |
S. aureus; nail-biting/trauma; warm soaks, flucloxacillin if cellulitis |
| 🦠 Paronychia (chronic) |
Swollen, boggy nail folds; ridging |
Irritant wet work; Candida colonisation; topical steroid + antifungal, avoid wet work |
| 💛 Yellow nail syndrome |
Yellow, thick, slow-growing, onycholysis |
Lymphoedema, pleural effusions, bronchiectasis; manage systemic disease |
| 🎯 Subungual melanoma |
New/widening pigmented band, irregular; Hutchinson sign |
Thumb/great toe common; urgent 2WW derm referral |
| 🧠 Habit-tic / median canaliform dystrophy |
Central longitudinal split/“fir-tree” ridging (thumbs) |
Repeated picking/pressure; behavioural advice, tape barrier |
| 🧴 Leukonychia |
White patches/lines in nail plate |
Trauma most common; true vs apparent; generally grows out |