
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Basics of Endocrinology
🧬 Endocrinology is the study of hormones-chemical messengers released into the blood to coordinate growth, metabolism, reproduction, fluid balance, calcium homeostasis, and stress responses. The core physiology is feedback control: endocrine systems behave like thermostats, using negative feedback to keep variables (glucose, osmolality, calcium, cortisol) within safe ranges, with pulsatile and circadian rhythms layered on top. In UK practice, “endocrine basics” is also about interpreting common tests sensibly (e.g., TSH-first for suspected primary hypothyroidism) and recognising when patterns imply pituitary disease or urgent pathology. (NICE CKS thyroid testing approach: check TSH first, then FT4 if raised.) ([cks.nice.org.uk](https://cks.nice.org.uk/topics/hypothyroidism/diagnosis/assessment/))
1) What makes a hormone “endocrine”?
- Endocrine: secreted into bloodstream to act at distant targets.
- Paracrine: acts on neighbouring cells (local signalling).
- Autocrine: acts back on the secreting cell.
- Neuroendocrine: neurons release hormones into blood (e.g., hypothalamic releasing hormones).
2) Hormone chemistry and receptors (how signals work)
- Peptide/protein hormones (e.g., insulin, ACTH, TSH):
- Water-soluble; circulate largely unbound; short half-life.
- Bind cell-surface receptors → second messengers (cAMP, IP3/DAG) → rapid effects.
- Steroid hormones (e.g., cortisol, aldosterone, oestradiol, testosterone):
- Lipid-soluble; circulate bound to proteins (CBG/albumin/SHBG); longer half-life.
- Bind intracellular receptors → gene transcription → slower onset, longer duration.
- Amine hormones:
- Catecholamines (adrenaline/noradrenaline): behave like peptides (surface receptors; rapid).
- Thyroid hormones (T3/T4): behave like steroids (nuclear receptors; slow genomic effects).
3) Feedback control and endocrine “axes”
Most major systems run as an axis: hypothalamus → pituitary → peripheral gland, with the peripheral hormone feeding back to suppress further release. This structure stabilises physiology but creates classic diagnostic patterns: if the peripheral hormone is low, the pituitary signal should rise (unless the pituitary/hypothalamus is the problem). TeachMePhysiology summarises this “axis” framework and feedback logic across pituitary systems. ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/anterior-pituitary-endocrine-function/))
- Negative feedback: cortisol inhibits CRH and ACTH (HPA axis). ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/hpa-axis/))
- Positive feedback (rare): high oestrogen (without progesterone) drives LH surge mid-cycle. ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/hypothalamic-pituitary-gonadal-axis/))
- Rhythms:
- Circadian: cortisol peaks in the early morning → why “9am cortisol” matters clinically.
- Pulsatile: GnRH pulses are essential-continuous GnRH suppresses LH/FSH (used therapeutically).
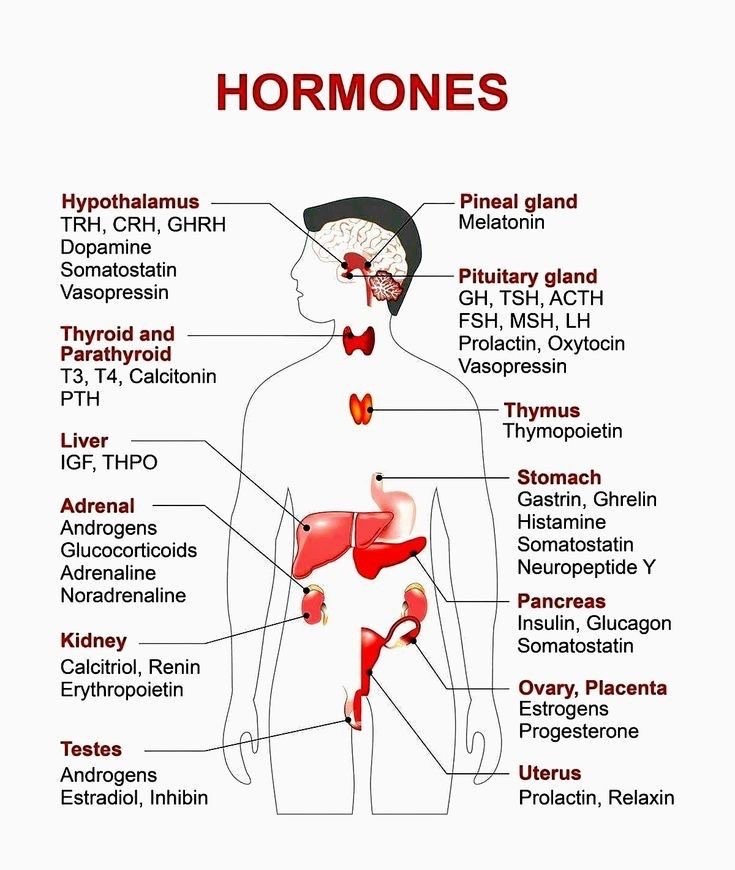
4) Endocrine anatomy: the major glands (where they are and what they do)
Endocrine glands secrete hormones directly into blood. NHS endocrine services commonly list the major glands as pituitary, thyroid, pancreas, adrenals, ovaries and testes (with parathyroids also central for calcium regulation). ([england.nhs.uk](https://www.england.nhs.uk/commissioning/spec-services/npc-crg/group-a/specialised-endocrinology/))
| Gland/organ | Location (anatomy) | Main hormones | Headline physiological role |
|---|---|---|---|
| Hypothalamus | Base of brain (diencephalon), above pituitary stalk | CRH, TRH, GnRH, GHRH, somatostatin, dopamine | Sets pituitary output; integrates stress, sleep, appetite, temperature |
| Pituitary (anterior/posterior) | Sella turcica; connected by infundibulum | TSH, ACTH, LH/FSH, GH, prolactin; (posterior releases ADH, oxytocin) | “Master gland” coordinating thyroid/adrenal/gonadal axes |
| Thyroid | Anterior neck, below larynx | T4/T3; calcitonin | Basal metabolic rate, thermogenesis, cardiac output, growth/neurodevelopment |
| Parathyroids | Usually 4 glands on posterior thyroid | PTH | Calcium/phosphate balance (bone–kidney–gut via vitamin D) |
| Adrenal cortex | On top of kidneys | Aldosterone, cortisol, androgens (DHEA) | Salt/water and BP (RAAS), stress metabolism, immune modulation |
| Adrenal medulla | Central adrenal (chromaffin cells) | Adrenaline/noradrenaline | Acute stress response (“fight/flight”) |
| Pancreatic islets | Within pancreas (esp. tail) | Insulin, glucagon, somatostatin | Glucose homeostasis (fed vs fasting metabolism) |
| Gonads | Ovaries/testes | Oestrogens, progesterone, testosterone; inhibin | Fertility, secondary sexual characteristics, bone and muscle effects |
The Endocrine Society provides a patient-friendly overview of endocrine organs and hormones that aligns with this gland-based map of endocrine function. ([endocrine.org](https://www.endocrine.org/patient-engagement/endocrine-library/hormones-and-endocrine-function))
5) “Big 5” endocrine physiology systems (high-yield core)
5.1 Glucose regulation (insulin–glucagon)
- Fed state: insulin promotes glucose uptake (muscle/adipose), glycogen synthesis, lipogenesis, and inhibits gluconeogenesis/ketogenesis.
- Fasting state: glucagon drives hepatic glycogenolysis and gluconeogenesis; later ketogenesis supports brain energy supply.
- Clinical physiology pearl: hypoglycaemia symptoms are partly adrenergic (sweat, tremor) from catecholamine response, and partly neuroglycopenic (confusion, seizures).
5.2 Thyroid axis (TRH → TSH → T4/T3)
- Thyroid hormone action: increases mitochondrial activity and Na/K ATPase expression → ↑ heat production and metabolic rate; sensitises heart to catecholamines.
- Feedback: high T3/T4 suppress TRH and TSH. ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/thyroid-stimulating-hormone/))
- UK testing principle: suspected primary hypothyroidism-check TSH first, then FT4 if TSH is raised (pattern recognition for primary vs secondary disease). ([cks.nice.org.uk](https://cks.nice.org.uk/topics/hypothyroidism/diagnosis/assessment/))
- NICE thyroid guideline context: NICE describes TFTs as widely used first-line biochemical tests for thyroid disorders. ([nice.org.uk](https://www.nice.org.uk/guidance/ng145/evidence/c-thyroid-function-tests-pdf-6967421679))
5.3 HPA axis (CRH → ACTH → cortisol)
- Cortisol: maintains BP responsiveness to catecholamines, promotes gluconeogenesis, and is immunomodulatory.
- Negative feedback: cortisol suppresses CRH and ACTH. ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/hpa-axis/))
- Clinical physiology pearl: cortisol’s circadian rhythm means timing matters-“random” cortisol can mislead unless interpreted in context.
5.4 Salt/water and BP (RAAS + ADH)
- RAAS: renal hypoperfusion → renin → angiotensin II → aldosterone → sodium retention and potassium excretion (volume and BP support).
- ADH (vasopressin): released from posterior pituitary; increases collecting duct water reabsorption → concentrated urine and osmolality control.
- Clinical physiology pearl: hyperkalaemia and metabolic acidosis can be clues to hypoaldosteronism (Addison’s, hyporeninaemic hypoaldosteronism).
5.5 Calcium homeostasis (PTH–vitamin D–bone/kidney)
- PTH: increases serum calcium by mobilising calcium from bone, increasing renal calcium reabsorption, and stimulating 1α-hydroxylase → active vitamin D.
- Vitamin D: increases gut calcium absorption; deficiency drives secondary hyperparathyroidism.
- Clinical physiology pearl: symptoms of hypocalcaemia (tetany, QT prolongation) reflect increased neuronal excitability; hypercalcaemia causes “stones, bones, groans…” via renal, skeletal and GI effects.
6) Endocrine investigation basics (UK pattern-recognition)
- Always interpret hormones with their “controller”:
- Low peripheral hormone + high pituitary hormone → primary gland failure (e.g., low FT4 + high TSH).
- Low peripheral hormone + low/normal pituitary hormone → secondary (pituitary/hypothalamic) disease.
- Timing matters (circadian/pulsatile hormones):
- Cortisol/ACTH and testosterone have diurnal patterns; prolactin can rise with stress.
- Binding proteins matter:
- Total hormone levels may change with altered binding proteins (pregnancy, oestrogen therapy); “free” hormones are usually more biologically meaningful (e.g., FT4).
Summary
Endocrinology is fundamentally about communication + control: glands release hormones, target tissues respond via receptors, and feedback loops stabilise internal physiology. The anatomical map (hypothalamus/pituitary/thyroid/parathyroids/adrenals/pancreas/gonads) links directly to the physiological “big systems” (glucose, metabolism, stress, BP/osmolality, calcium). Clinically, most endocrine reasoning reduces to axis logic (primary vs secondary patterns) plus rhythm-aware test interpretation-exactly why NICE CKS emphasises structured approaches such as TSH-first in suspected primary hypothyroidism. ([cks.nice.org.uk](https://cks.nice.org.uk/topics/hypothyroidism/diagnosis/assessment/))
References
- NHS England (Specialised endocrinology): endocrine glands and examples. ([england.nhs.uk](https://www.england.nhs.uk/commissioning/spec-services/npc-crg/group-a/specialised-endocrinology/))
- Endocrine Society: Hormones and endocrine function (overview). ([endocrine.org](https://www.endocrine.org/patient-engagement/endocrine-library/hormones-and-endocrine-function))
- Endocrine Society: Brain hormones (hypothalamus/pituitary as controllers). ([endocrine.org](https://www.endocrine.org/patient-engagement/endocrine-library/hormones-and-endocrine-function/brain-hormones))
- TeachMePhysiology: Anterior pituitary endocrine function (axis/feedback framework). ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/anterior-pituitary-endocrine-function/))
- TeachMePhysiology: HPA axis (negative feedback). ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/hpa-axis/))
- TeachMePhysiology: HPG axis (feedback including LH surge concept). ([teachmephysiology.com](https://teachmephysiology.com/endocrine-system/hypothalamus-pituitary/anterior-pituitary/hypothalamic-pituitary-gonadal-axis/))
- NICE CKS: Hypothyroidism - Assessment (TSH-first approach for suspected primary hypothyroidism). ([cks.nice.org.uk](https://cks.nice.org.uk/topics/hypothyroidism/diagnosis/assessment/))
- NICE NG145 evidence: Thyroid function tests (background on TFTs as first-line biochemical tests). ([nice.org.uk](https://www.nice.org.uk/guidance/ng145/evidence/c-thyroid-function-tests-pdf-6967421679))
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery