Nephrotic Syndrome in Children ✅
Related Subjects:
|Encopresis in Children
|Enuresis/Bedwetting in Children
|Acute Glomerulonephritis in Children
|Nephrotic Syndrome in Children
|Acute Appendicitis in Children
|Gastro-oesophageal reflux in Children
|Intussusception in Children
|Panayiotopoulos Syndrome in Children
|Reflex anoxic attacks in Children
🧒 Nephrotic syndrome (children) occurs when podocyte injury leads to heavy protein loss in urine 🩸➡️💧.
Loss of albumin lowers plasma oncotic pressure → oedema 💧, while effective circulating volume may be low.
The liver responds with hyperlipidaemia 🧈, and loss of anticoagulants (e.g., antithrombin) increases thrombosis risk 🩸.
✅ Definition (typical paediatric nephrotic syndrome)
- Generalised oedema 💧
- Nephrotic-range proteinuria: urine PCR >200 mg/mmol 🧪
- Hypoalbuminaemia: albumin <25 g/L ⬇️
- Hyperlipidaemia 🧈 (supportive, not required for diagnosis)
⚠️ Causes (childhood)
- Idiopathic nephrotic syndrome (mostly Minimal Change Disease) ✅
- Secondary: infection, SLE/HSP, drugs, malignancy (less common)
- Other glomerular diseases with nephrotic-range proteinuria ± nephritic features
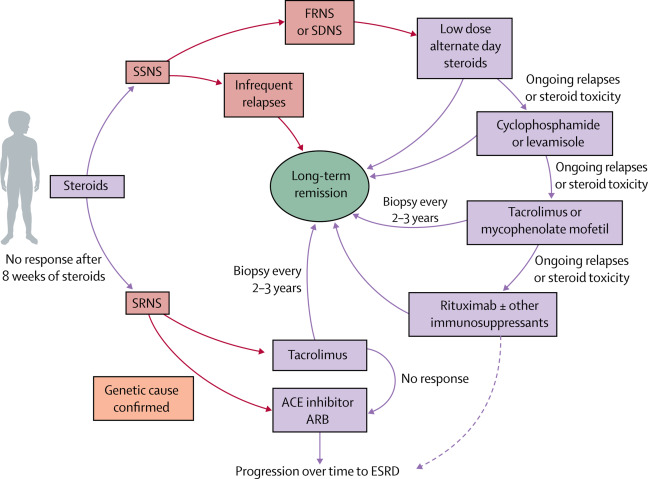
🧾 Clinical pattern categories
- ✅ Steroid-sensitive (SSNS) – remission with standard prednisolone course (1–4 weeks)
- ♻️ Steroid-dependent (SDNS) – relapse during taper or soon after stopping steroids
- ❌ Steroid-resistant (SRNS) – failure to remit with initial steroid course; specialist pathway/biopsy required
🤒 Symptoms & signs
- Oedema: periorbital 👁️ → generalised (legs, ascites, scrotal/vulval)
- Weight gain ⚖️, lethargy, reduced urine output 🚱
- Frothy urine ☁️ (protein)
- Red flags: abdominal pain, fever, breathlessness, severe headache, cool peripheries 🚨
🔬 Investigations (first presentation)
- Urine: PCR/ACR, dipstick (blood), culture if febrile; microscopy as indicated
- Bloods: U&E/creatinine, albumin, cholesterol, FBC, CRP; LFTs if needed
- Atypical feature screen: complement (C3/C4), ANA, infection screens as indicated
- Renal biopsy: atypical features, steroid resistance, age extremes, systemic features (specialist decision)
🩺 General management (key points)
- Early paediatric nephrology involvement 👩⚕️👨⚕️
- Salt restriction 🧂⬇️ (effective for oedema)
- Fluid management 💧 – assess intravascular volume carefully
- Diuretics 💊 – specialist-guided only (risk of hypovolaemia/AKI)
- Albumin infusion 💉 – severe/refractory oedema under specialist protocol
- Daily weight ⚖️ and oedema charting
- Avoid NSAIDs 🚫 (renal perfusion risk)
💊 Prednisolone for first presentation (common UK regimen)
- 60 mg/m²/day (max 60–80 mg) for 4 weeks
- 40 mg/m² alternate days for 4 weeks
- Taper: 5–10 mg/m² alternate days weekly over ~4 weeks 📉
- Most SSNS children achieve remission early ✅
🧯 Relapse & escalation
- Relapses are common; management guided by relapse frequency & steroid toxicity
- Frequent relapses / SDNS: steroid-sparing agents (levamisole, cyclophosphamide, calcineurin inhibitors) via nephrology
- SRNS: specialist pathway + biopsy; consider ACEi/ARB for proteinuria reduction
⚠️ Complications to monitor
- Infections 🦠 (pneumococcal, cellulitis, peritonitis)
- Hypovolaemia / shock 🚨 (tachycardia, cool peripheries, abdominal pain, oliguria)
- AKI 🩺 (from hypovolaemia, sepsis, nephrotoxins)
- Thrombosis / VTE 🩸 (abdominal pain, haematuria, chest symptoms, limb swelling)
💉 Vaccines & infection prevention (UK)
- Routine immunisations up to date ✅
- Annual influenza vaccine 🦠➡️💉
- Pneumococcal vaccination/boosters per local pathway 💉
- Check varicella status; manage exposure carefully if immunosuppressed
- Avoid live vaccines during high-dose steroids & shortly after stopping
📚 References
-
NHS Greater Glasgow & Clyde (NHS Scotland). Idiopathic nephrotic syndrome: management in children.
View guideline
-
infoKID (UK paediatric kidney information). Nephrotic syndrome.
View infoKID page
