Related Subjects:
|Fracture management basics
|Fractured Neck of Femur
|Fractured Shaft Femur
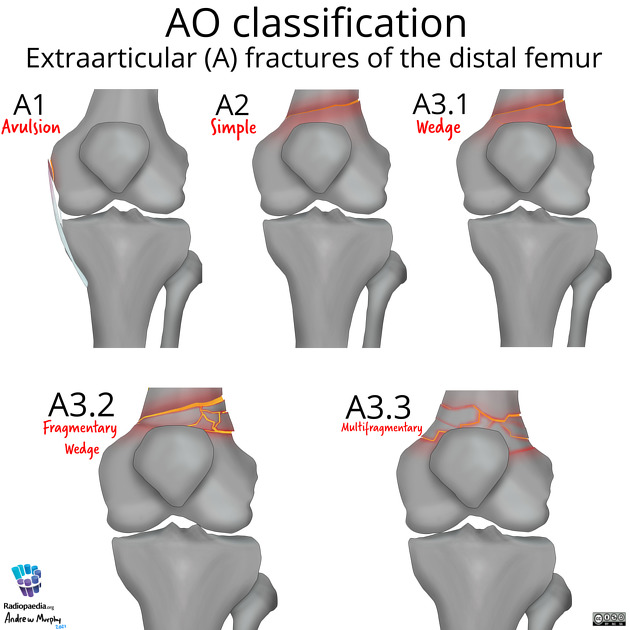
|Fractured Femur Supracondylar Fractures
|Fractured Femur
|Fractured Tibia and Fibula
Supracondylar Femur Fractures 🦴 occur just above the knee joint.
They are uncommon but serious, often from high-energy trauma (RTAs, falls) or low-energy in elderly/osteoporotic bone.
These fractures may involve the articular surface and carry a risk of knee stiffness, malunion, and post-traumatic arthritis.
📖 About
- Unusual fracture located in the distal femur, just proximal to the condyles.
- Seen in young adults after high-energy trauma and in elderly patients with osteoporosis after low-energy falls.
- May occur above a total knee replacement (periprosthetic fracture).
⚙️ Aetiology
- High-force injuries: RTAs, falls from height, sports accidents.
- Low-force in osteoporotic or pathological bone.
- Fracture line may extend into knee articular cartilage → ↑ risk of arthritis.
🩺 Clinical Features
- Severe localised pain, swelling, deformity of distal thigh/knee.
- Unable to bear weight 🚶❌.
- Check for neurovascular compromise:
- Femoral/popliteal artery injury → absent pulses.
- Peroneal/tibial nerve injury → motor/sensory deficit.
- Look for compartment syndrome signs 🚨.
🧪 Investigations
- X-rays: AP & lateral of femur, including hip and knee.
- CT: for intra-articular extension or surgical planning.
- Bloods: trauma panel (FBC, U&E, coagulation, group & save).
⚠️ Complications
- Malunion / nonunion.
- Vascular injury: femoral or popliteal artery damage → limb-threatening.
- Compartment syndrome of the thigh/leg.
- Fat embolism (esp. young adults with long bone fractures).
- Venous thromboembolism (DVT/PE).
- Osteomyelitis (esp. open fractures).
- Post-traumatic knee arthritis (if articular involvement).
💊 Management
- Initial (ATLS): ABCDE, IV access, fluids, analgesia.
Check distal pulses + neurology. Splint limb, apply sterile dressings to wounds.
- Open fractures 🚨: IV antibiotics (e.g., co-amoxiclav or clindamycin), tetanus prophylaxis, urgent ortho referral for debridement + fixation.
- Definitive management:
- Usually operative:
- Intramedullary nail (retrograde via knee or antegrade via hip).
- Locking plate fixation for comminuted/osteoporotic bone.
- External fixation as temporary measure in polytrauma or open fractures.
- Above a total knee replacement:
- If prosthesis stable → fixation around it.
- If loose → revision arthroplasty may be required.
- Rehabilitation: early physiotherapy, progressive weight-bearing depending on fixation stability.
- VTE prophylaxis: LMWH unless contraindicated.
📌 OSCE / Exam Pearls
- Always assess neurovascular status in distal femur fractures (femoral/popliteal artery at risk).
- Periprosthetic supracondylar fracture is a classic viva question → may require revision TKR if implant loose.
- Think “high force in young, low force in elderly.”
- CT often needed to define intra-articular extension.
📚 References
- ATLS®: Advanced Trauma Life Support, 10th edition.
- Rockwood & Green’s Fractures in Adults, 9th edition.
- BOAST Guidelines: Distal Femur Fractures.