Related Subjects:
|Assessing Breathlessness
|Pulmonary Embolism
|Deep Vein Thrombosis
|DVT/PE in pregnancy
|CTPA
📖 Introduction
- CT pulmonary angiography (CTPA) is the first-line imaging test in most adults when pulmonary embolism (PE) is suspected and imaging is required after clinical risk stratification.
- The usual diagnostic pathway is: clinical probability assessment (for example Wells score) → D-dimer if low/intermediate probability → CTPA if D-dimer positive or clinical probability is high.
- CTPA uses a rapid intravenous bolus of iodinated contrast timed to opacify the pulmonary arterial tree.
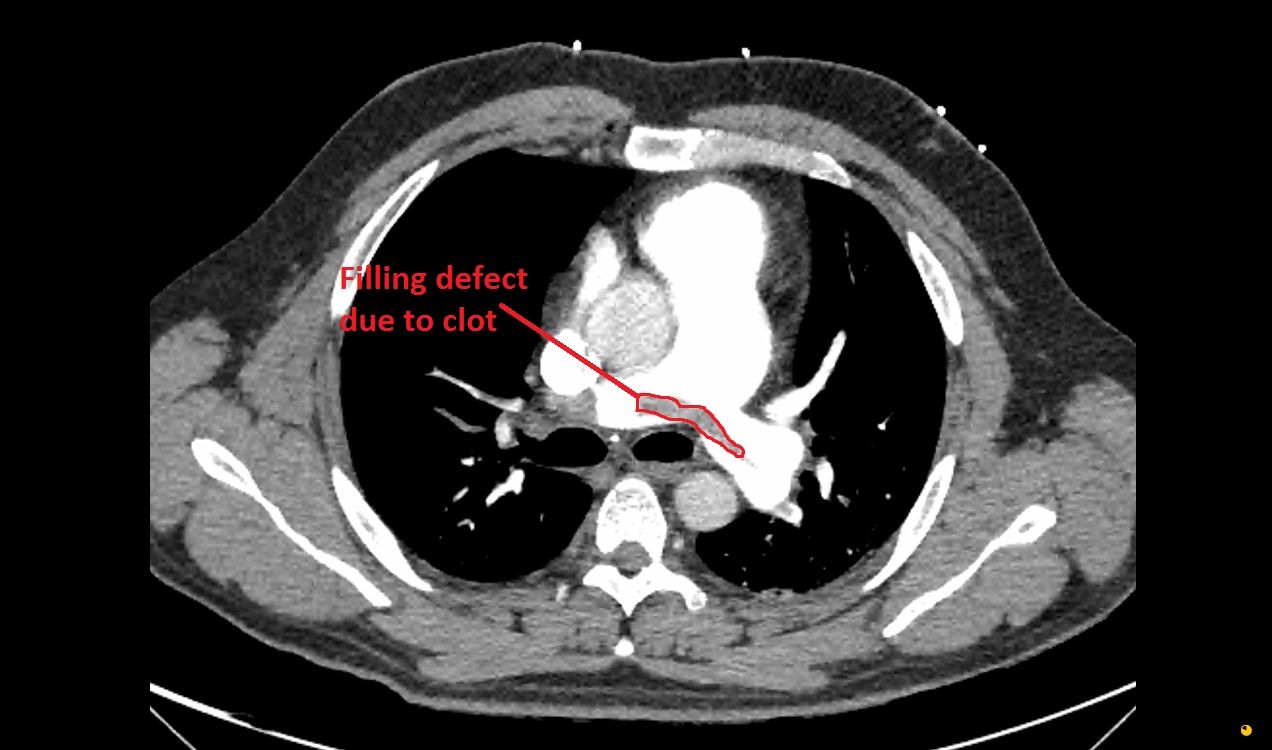
- An acute PE appears as a low-attenuation intraluminal filling defect within a contrast-opacified pulmonary artery.
- CTPA can also reveal alternative diagnoses such as pneumonia, pleural effusion, pneumothorax, malignancy, or aortic pathology.
🖥️ What CTPA Shows
- After contrast injection, the normal pulmonary arteries should appear bright and uniformly opacified.
- An embolus is seen as a darker filling defect within the vessel lumen because contrast cannot occupy the space taken up by thrombus.
- Acute thrombus may be:
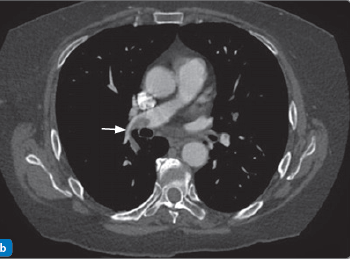
- Central within the lumen, surrounded by contrast - producing the classic “polo mint” sign on axial views or “railway track” sign on longitudinal views.
- Eccentric and wall-adherent, partially narrowing the lumen.
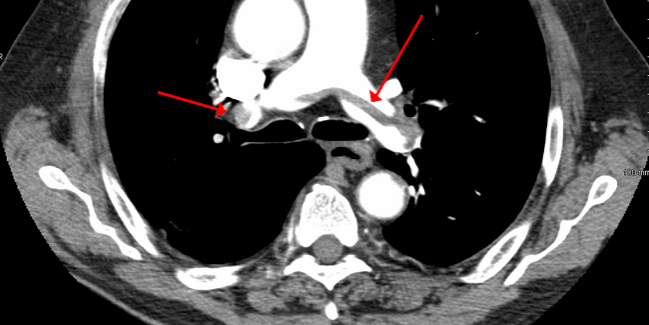
- Occlusive, causing abrupt vessel cut-off.
- A large clot may straddle the bifurcation of the main pulmonary artery, forming a saddle embolus.
- More distal emboli may be seen in lobar, segmental, or subsegmental branches.
- Acute PE usually forms acute angles with the vessel wall, whereas chronic thrombus is more often eccentric, forms obtuse angles, and may be associated with webs, bands, or vessel narrowing.
📈 Why CTPA Matters Beyond Diagnosis
- CTPA not only confirms or excludes PE, but also provides important risk-stratification information.
- Features suggesting right ventricular (RV) strain include:
- RV enlargement, often with an RV:LV ratio >1
- Interventricular septal flattening or bowing towards the left ventricle
- Reflux of contrast into the IVC or hepatic veins
- Main pulmonary artery dilatation
- These signs indicate acute pressure overload and are associated with a worse short-term prognosis.
- CTPA may also show complications such as pulmonary infarction, pleural effusion, or atelectatic change.
🧭 Systematic Approach: How to Read a CTPA
- ✅ Check technical quality first: are the pulmonary arteries bright and well-opacified? If contrast timing is poor, the study may be non-diagnostic.
- ✅ Start centrally: inspect the main pulmonary artery, then the right and left pulmonary arteries.
- ✅ Track distally: follow each vessel into the lobar → segmental → subsegmental branches.
- ✅ Look for filling defects: sharply defined darker areas within contrast suggest thrombus.
- Central clot surrounded by contrast = polo mint sign
- Linear clot seen on sagittal/coronal reformats = railway track sign
- Eccentric wall-adherent defect = partial obstruction
- ✅ Assess the heart: look for RV enlargement, septal bowing, and contrast reflux into the IVC/hepatic veins.
- ✅ Review the lung windows: look for wedge-shaped pleural-based infarcts, consolidation, collapse, masses, or emphysema.
- ✅ Review mediastinum and pleura: do not miss pleural effusions, lymphadenopathy, pneumothorax, or aortic pathology.
- ✅ Do a final top-to-bottom sweep: scroll from apices to bases to reduce the risk of missing peripheral emboli.
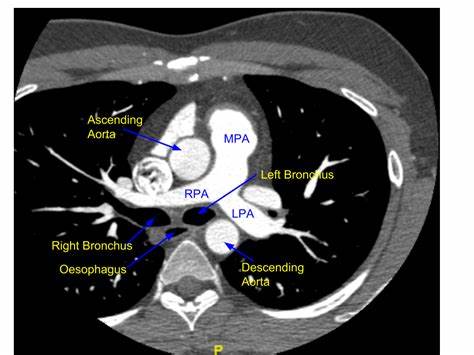
🫁 Pulmonary Artery Anatomy
- The main pulmonary artery arises from the right ventricle and bifurcates into:
- Right pulmonary artery (RPA) - passes more horizontally towards the right lung
- Left pulmonary artery (LPA) - arches posteriorly towards the left lung
- These vessels then divide into lobar, segmental, and subsegmental branches.
- A normal CTPA shows smooth, uninterrupted contrast opacification throughout the pulmonary arterial tree.
🩺 Common Secondary Findings
- Pulmonary infarction - often a peripheral, wedge-shaped pleural-based opacity.
- Pleural effusion - usually small and reactive.
- Atelectasis - common but non-specific.
- Alternative pathology - pneumonia, malignancy, pneumothorax, interstitial lung disease, or aortic disease.
⚠️ Contraindications / Limitations
- 🤰 Pregnancy: choice of imaging depends on gestation, chest X-ray findings, and local protocol; V/Q scanning may be preferred in some cases.
- 💧 Renal impairment: iodinated contrast may not be suitable in significant renal dysfunction; check renal function and weigh risk versus benefit.
- ⚠️ Contrast allergy: severe previous contrast reactions may preclude CTPA; alternatives include V/Q scanning.
- 💓 Haemodynamic instability: some patients are too unstable to leave the resuscitation area; bedside echo and emergency management may take priority.
- 🌫️ Suboptimal scan quality: motion artefact, poor breath-holding, and poor contrast bolus timing can limit interpretation.
📌 Practical Pitfalls
- ⏱️ Poor opacification: inadequate contrast timing can create a falsely reassuring scan or obscure small emboli.
- 💨 Respiratory motion artefact: may mimic filling defects, especially centrally.
- ❤️ Cardiac motion: can degrade assessment of vessels near the heart.
- 📍 Subsegmental PE: small peripheral emboli can be difficult to distinguish from artefact and must be interpreted in clinical context.
- 🧩 Non-thrombotic mimics: tumour emboli, flow artefact, mucus plugging adjacent to vessels, and beam-hardening artefact may confuse interpretation.
- 🔍 Satisfaction error: once one embolus is found, additional emboli and signs of RV strain may be overlooked.
💡 Teaching Pearls
1️⃣ Always assess scan quality before looking for PE.
2️⃣ Use a central → lobar → segmental → subsegmental search pattern every time.
3️⃣ A PE is a filling defect in a contrast-filled artery.
4️⃣ Do not stop at “PE present” - always assess for RV strain, as this changes risk.
5️⃣ Always review lung windows, pleura, and mediastinum for infarction or alternative diagnoses.
6️⃣ A negative CTPA does not overrule the clinical picture if the scan is poor quality or suspicion remains very high.
🎓 Reporting Language to Recognise
- “Central filling defect” = thrombus seen within the opacified artery.
- “Saddle embolus” = clot across the main pulmonary artery bifurcation.
- “RV strain” = imaging evidence of acute right heart pressure overload.
- “Peripheral wedge-shaped opacity” = likely pulmonary infarction.
- “No convincing PE, but limited by motion / poor opacification” = technically suboptimal scan; interpret with caution.
🎥 Online Learning
🩻 CTPA Images