
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
ECG - P wave
🌊 Normal P Wave
- Shape: Smooth, rounded in most leads (esp. I & II) ➝ reflects coordinated atrial depolarisation.
- Duration: ⏱️ 0.08–0.11 sec (80–110 ms). >0.12 sec suggests atrial conduction delay / enlargement.
- Amplitude: 📏 <2.5 mm in lead II. >2.5 mm often = right atrial enlargement (P pulmonale).
- Direction:
- ✅ Upright: Leads I, II, aVL, aVF
- ❌ Inverted: Lead aVR
- ↔️ Biphasic: Lead V1 (right vs left atrial contributions)
- Physiological Significance: 🫀 Represents atrial depolarisation from SA node → atria.
⚠️ Abnormal P Waves
| Abnormality | Cause | ECG Appearance |
|---|---|---|
| Peaked P (P Pulmonale) | Right atrial enlargement (e.g. pulmonary HTN, COPD) | 📈 Tall >2.5 mm in lead II |
| Broad/Notched (P Mitrale) | Left atrial enlargement (mitral valve disease, LVH) | ⏱️ >0.12 sec, notched "M-shaped" P in I, II |
| Inverted P | Ectopic atrial / junctional rhythm | ↘️ P inverted in leads normally upright (I, II) |
| Absent P | Atrial fibrillation, AV junctional rhythm | 🌀 No P; fibrillatory baseline in AF |
| Prolonged P | Left atrial enlargement, interatrial block | ⏱️ P >0.12 sec in I, II |
| Varying Morphology | Multifocal atrial tachycardia (MAT), wandering pacemaker | 🎭 ≥3 different P morphologies |
| P Wave Axis Deviation | Atrial enlargement / conduction abnormality | 📐 Abnormal axis → unexpected inversion |
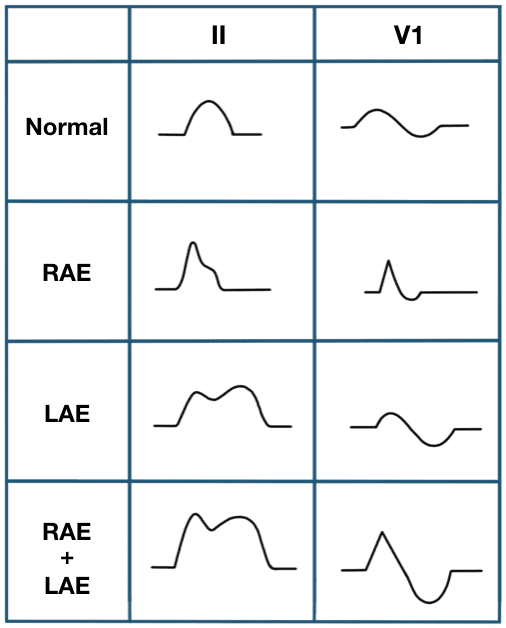
💡 Clinical Pearl: 👉 In practice, always check P wave morphology in lead II and V1 first: - Lead II = tells you size (RAE/LAE). - Lead V1 = tells you phase balance (RA vs LA). 🔑 Subtle P wave changes often give the first clue to atrial disease.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery