Cryptococcus neoformans infections (Cryptococcal Infections)
Related Subjects:
|Lumbar Puncture
|CSF Interpretation
💡 CSF may be normal or only mildly abnormal in cryptococcal meningitis. Opening pressure is often high due to impaired CSF absorption at the arachnoid granulations. The higher the fungal burden, the higher the pressure. Cryptococcal antigen testing is essential for diagnosis.
📖 About
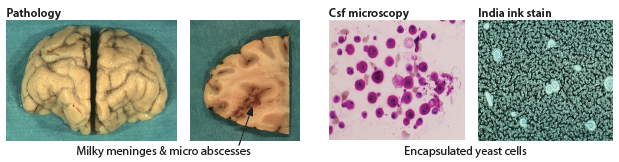
- Cryptococcosis is a serious opportunistic fungal infection caused by an encapsulated yeast (Cryptococcus neoformans or Cryptococcus gattii).
- 🧪 The yeast is 2–15 µm, surrounded by a sugar-rich capsule that blocks immune clearance.
- It can cause pneumonia, but CNS infection (meningitis ± space-occupying lesions) is the most feared presentation.
- High morbidity and mortality → requires prompt antifungal therapy and ICP control.
🧬 Aetiology
- 🌱 Acquired by inhalation of spores from bird droppings (especially pigeons) or contaminated soil.
- Starts as a pulmonary infection, then spreads haematogenously to the CNS and other organs.
- Classically seen in patients with impaired cell-mediated immunity (HIV/AIDS, transplant, malignancy, chronic steroids).
⚠️ At-Risk Groups
- HIV/AIDS with CD4 count < 100 (esp. < 50).
- Post-organ transplant (on immunosuppressants).
- Hematological malignancies.
- Chronic corticosteroid use, sarcoidosis.
🧾 Clinical Presentation
- Subacute onset (days–weeks) of headache, fever, malaise.
- Neurological: Basal meningitis → cranial nerve palsies, confusion, stroke-like events.
- Raised ICP: Severe headache, nausea, vomiting, blurred vision, papilloedema.
- Respiratory: Dry cough, fever, chest infiltrates; may cause ARDS in severe cases.
- Skin: Umbilicated papules resembling molluscum contagiosum.
- Other organ involvement: myocarditis, hepatitis, renal abscess, chorioretinitis.
🔎 Investigations
- Baseline: FBC, U&E, LFTs, CRP, HIV test with CD4 count and viral load. CXR for pulmonary focus.
- CT head before LP: In immunocompromised patients (exclude SOL/mass effect).
- CSF findings: High opening pressure, ↑protein, lymphocytosis, low/normal glucose.
- India Ink: Demonstrates encapsulated yeasts in ~90% of HIV patients.
- Cryptococcal Antigen (CrAg): Serum or CSF test – highly sensitive and specific.
- Culture: Yeast may grow from CSF, blood, urine, or sputum.
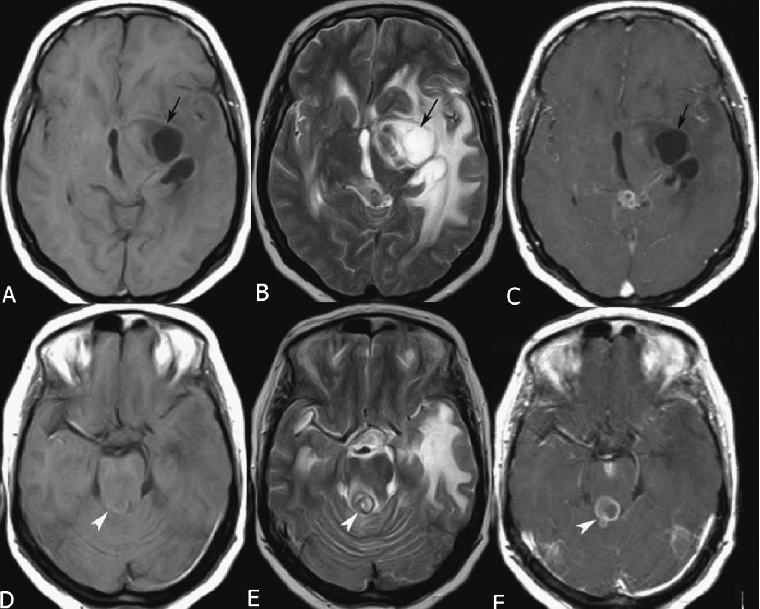
🧠 Imaging
- MRI/CT: May show cryptococcal abscesses (“gelatinous pseudocysts”), meningeal enhancement, or hydrocephalus.
💊 Management
- Induction Therapy: IV liposomal Amphotericin B + Flucytosine for 2 weeks. Monitor renal function and electrolytes closely (risk of nephrotoxicity, hypokalaemia, hypomagnesaemia).
- Consolidation Therapy: Switch to oral Fluconazole 400 mg daily for ≥8 weeks.
- Maintenance Therapy: Fluconazole 200 mg daily long-term in AIDS patients until CD4 recovery on HAART.
- HAART: In HIV-positive patients, start ~2 weeks after antifungals (to reduce risk of IRIS).
- ICP Control: Serial therapeutic lumbar punctures if opening pressure > 25 cmH₂O; in refractory cases, consider CSF shunt/ventricular drain.
- Supportive Care: Analgesia, antiemetics, correction of electrolytes, and careful fluid balance.
📊 Prognosis
- Untreated cryptococcal meningitis is almost universally fatal.
- With prompt antifungal therapy, mortality falls significantly, but relapse risk is high without maintenance therapy in immunocompromised patients.
