
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Wellens Syndrome
Related Subjects: |Atherosclerosis |Ischaemic heart disease |Assessing Chest Pain |Acute Coronary Syndrome (ACS): Complications |ACS - General |ACS - STEMI |ACS - NSTEMI |ACS - GRACE Score |ACS - ECG Changes |ACS -Cardiac Troponins |ACS - Post MI arrhythmias |ACS: Right Ventricular STEMI |ACS: Sgarbossa Criteria |Wellen's syndrome
⚠️ Because Wellens syndrome patients have critical narrowing of the LAD coronary artery, stress testing is contraindicated. It may precipitate acute MI and sudden cardiac death.
🔎 Introduction
- Wellens syndrome = a classic ECG pattern indicating imminent anterior MI due to critical LAD stenosis.
- Key to recognise in the ED – early intervention is lifesaving.
🧬 Aetiology
- Represents >90% stenosis of the LAD artery.
- Critical narrowing → high risk of complete occlusion & anterior wall STEMI.
⚙️ Pathophysiology
- Atherosclerotic plaque: High-grade LAD lesion causes intermittent reduced perfusion.
- Vasospasm: LAD spasm may contribute to transient ischaemia.
- Increased demand: Exercise/stress raises oxygen demand, worsening ischaemia.
- Hypoxia: Systemic hypoxaemia aggravates LAD compromise.
⚠️ Risk Factors
- Diabetes mellitus
- Hypertension
- Hyperlipidaemia / Hypercholesterolaemia
- Smoking
- Metabolic syndrome
- Family history of premature IHD
- Age & occupational stress
🧾 Clinical Presentation
- Chest pain (often anginal, may have settled by time of ECG).
- Anginal equivalents: arm pain, jaw pain, dyspnoea.
- May be asymptomatic → ECG is crucial.
📊 Investigations
- Bloods: FBC, U&E, LFTs, lipids.
- Troponin: May be normal or only mildly raised.
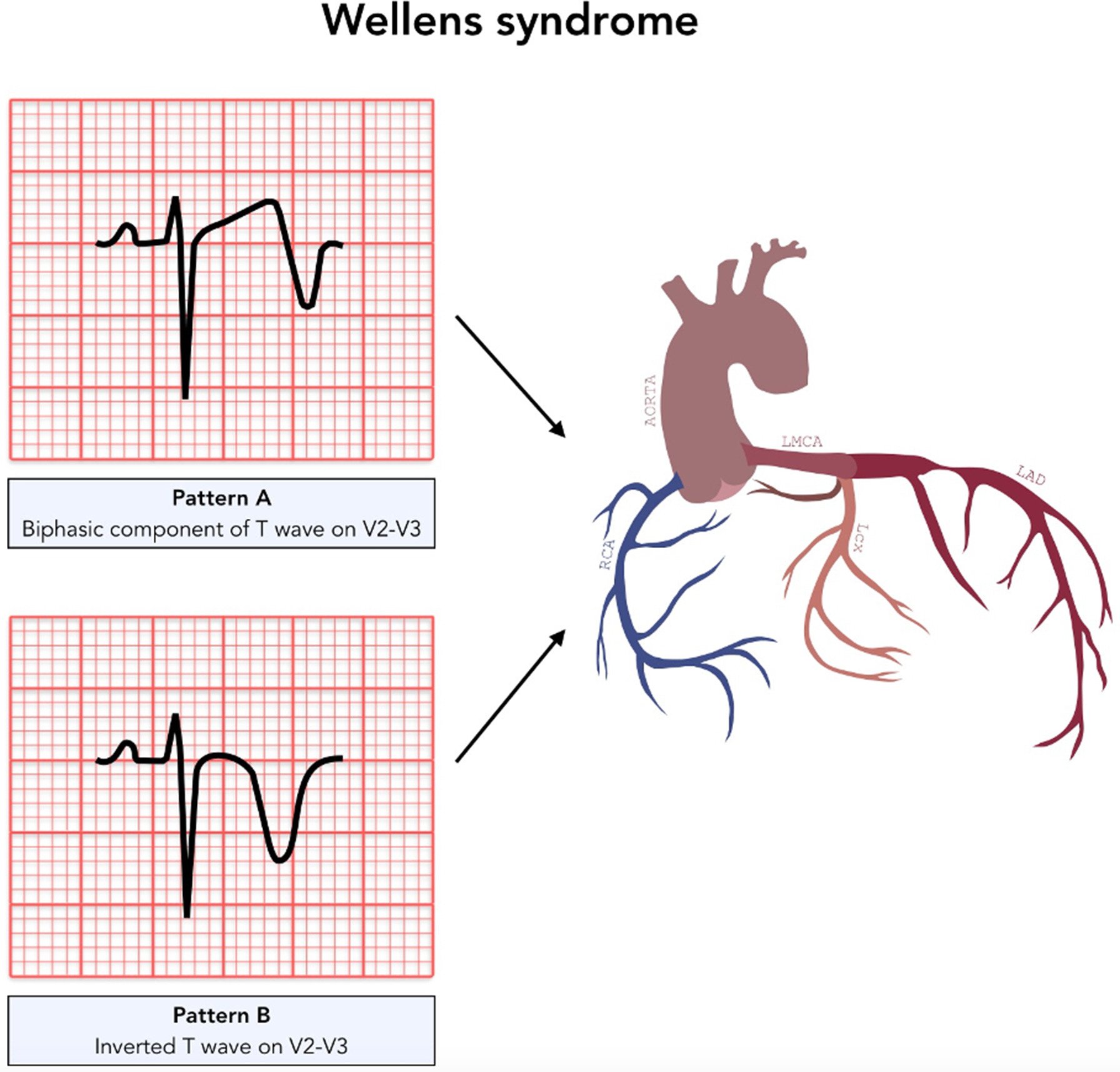
- ECG hallmarks:
- Biphasic or deeply inverted T waves in V2–V3.
- Can extend V1–V6 (critical LAD territory).
- T wave normalisation + hyperacute waves = impending STEMI.
- Echocardiogram: Wall motion abnormalities in anterior wall.
- Coronary angiography: Gold standard for diagnosis & management planning.
🩺 Management
- Immediate Care: Admit CCU, oxygen if hypoxic, aspirin/clopidogrel, nitrates, beta-blockers (if not contraindicated).
- STEMI protocol: If ST elevation develops → manage as acute STEMI.
- Definitive: Early coronary angiography → PCI or CABG depending on anatomy.
- Avoid stress testing: Contraindicated due to risk of precipitating full infarct.
📌 Prognosis & Clinical Significance
- Untreated → very high risk of anterior wall MI within days to weeks.
- Early recognition + PCI/CABG = excellent outcome.
- Secondary prevention vital: BP & cholesterol control, diabetes optimisation, smoking cessation, antiplatelet + statin therapy.
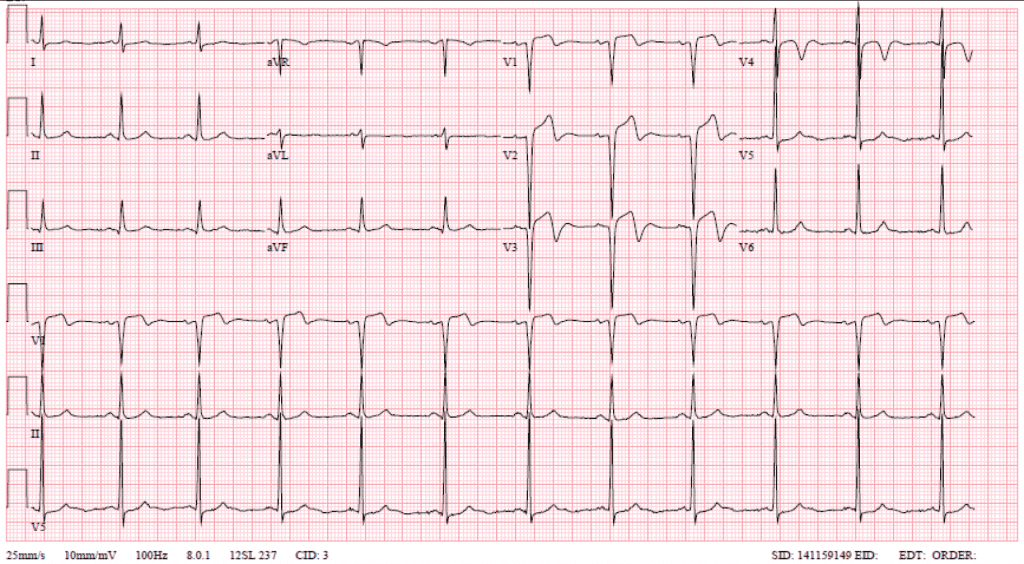
🖼️ Classic ECG Examples





📚 References
- Wellens Syndrome – NCBI Bookshelf
- de Zwaan C, Wellens HJ. “Characteristic electrocardiographic pattern indicating critical LAD stenosis.” Am Heart J. 1982.
Exam Pearl: – Wellens = T-wave changes in V2–V3 + critical LAD stenosis + pain-free at time of ECG. – Never stress test a Wellens patient 🚫🏃.
Cases - Wellens’ Syndrome
- Case 1 - Type A (biphasic T-waves) 📉: A 56-year-old man presents with intermittent central chest tightness over 2 days, now pain-free. ECG: biphasic T-waves in V2–V3, no ST elevation. Troponin mildly raised. Diagnosis: Wellens’ syndrome (critical LAD stenosis, Type A pattern). Managed with hospital admission, antiplatelets, and urgent coronary angiography ± PCI. ⚠️ Stress testing contraindicated due to risk of infarction.
- Case 2 - Type B (deeply inverted T-waves) ⚠️: A 63-year-old woman with diabetes presents with recent exertional angina, now pain-free in ED. ECG: deeply inverted, symmetrical T-waves in V2–V4, preserved R-wave progression. Troponin borderline. Diagnosis: Wellens’ syndrome (Type B pattern). Managed with dual antiplatelet therapy, heparin, and urgent revascularisation planning.
- Case 3 - Missed diagnosis → infarction 🚨: A 60-year-old man is discharged after presenting with atypical chest pain and “nonspecific T-wave changes.” Two days later he returns with severe chest pain. ECG: anterior ST-elevation MI. Angiography: complete proximal LAD occlusion. Retrospective review: prior ECG showed Wellens’ T-wave inversions. Diagnosis: progression of untreated Wellens’ syndrome to LAD infarction. Teaching point: always recognise the pattern!
Teaching Point 🩺: Wellens’ syndrome is a pre-infarction state caused by critical proximal LAD stenosis. ECG patterns (seen in pain-free state): - Type A: biphasic T-waves in V2–V3. - Type B: deeply inverted, symmetrical T-waves in anterior leads. No Q waves, no loss of R-wave progression, little ST elevation. ⚠️ High risk of extensive anterior MI → requires urgent angiography/PCI, not stress testing. Troponin may be normal or only mildly raised.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery