
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
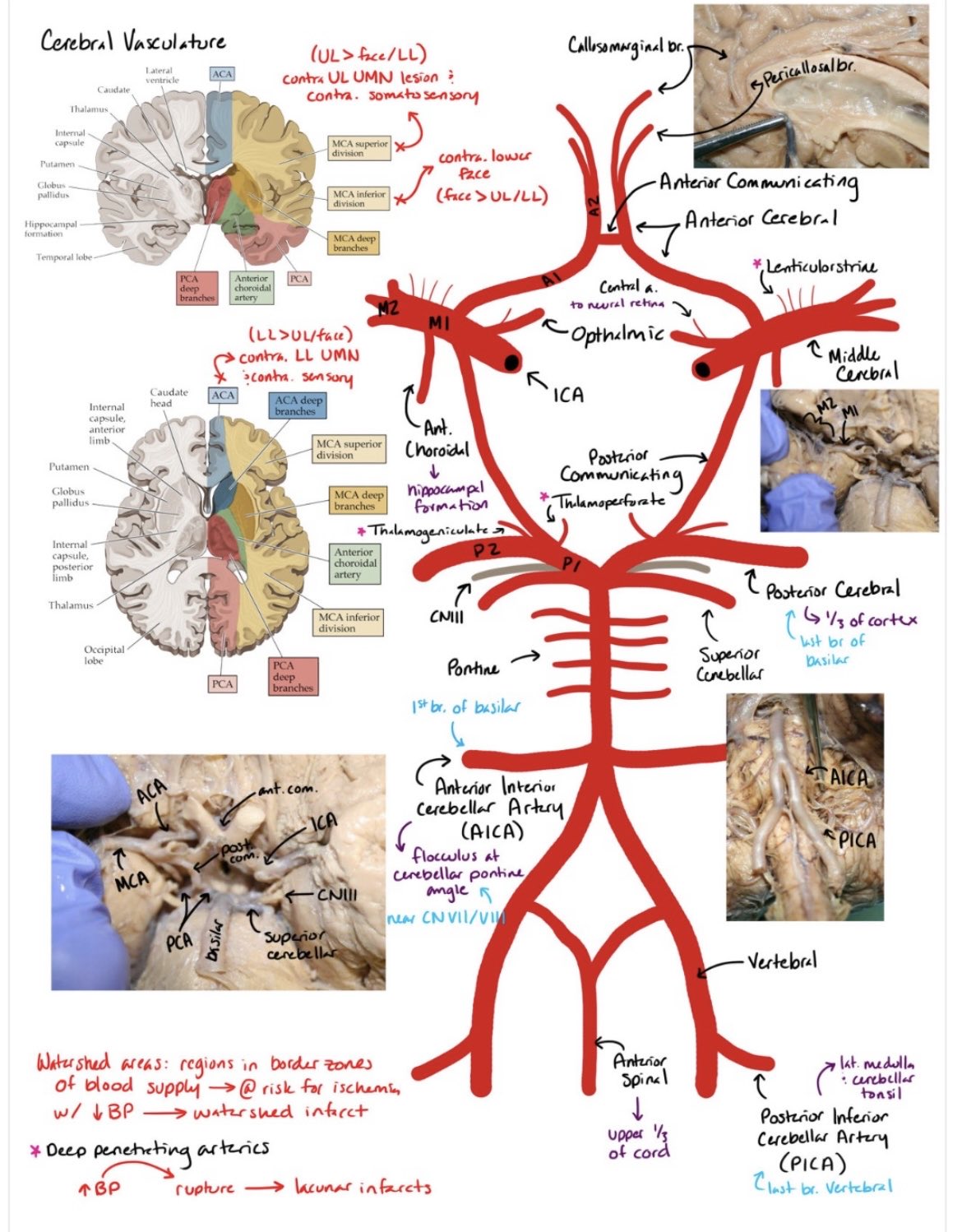
The Circle of Willis
The Circle of Willis is an arterial anastomotic ring at the base of the brain that provides collateral blood flow between the anterior and posterior circulations. Its primary role is haemodynamic resilience: maintaining cerebral perfusion if one major vessel is narrowed or occluded. In practice, its effectiveness depends heavily on anatomical completeness, which is highly variable.
🔗 Components of the Circle of Willis
The circle is formed by branches of the internal carotid and vertebrobasilar systems. It links left and right hemispheres and connects anterior and posterior circulations.
- Anterior cerebral arteries (A1 segments, left and right)
- Anterior communicating artery (ACom)
- Internal carotid arteries (terminal portions)
- Posterior communicating arteries (PCom, left and right)
- Posterior cerebral arteries (P1 segments, left and right)
🌊 Haemodynamic Function
Under normal conditions, flow across the communicating arteries is minimal. When pressure drops in one arterial territory, blood is redirected through the circle along pressure gradients. This explains why a complete circle can protect against ischaemia, while an incomplete circle may fail catastrophically.
⚠️ Common Anatomical Variants
A “textbook” complete Circle of Willis is present in a minority of individuals. Most people have at least one hypoplastic or absent segment, which has important clinical consequences.
- Hypoplastic or absent PCom: Reduced anterior–posterior collateral flow
- Hypoplastic A1 segment: One ACA supplies both hemispheres → risk in ICA disease
- Asymmetrical PCA origins: Alters posterior circulation perfusion
👶 Fetal Posterior Cerebral Artery (fPCA)
In the fetal configuration, the posterior cerebral artery arises predominantly from the internal carotid artery rather than the basilar artery. This persists into adulthood in a significant minority of patients. Clinically, this means ICA disease can cause occipital infarction, which would otherwise suggest posterior circulation pathology.
- PCA supplied mainly by ICA via large PCom
- P1 segment small or absent
- Important cause of “unexpected” visual field loss in ICA stroke
🩺 Clinical Relevance
Circle of Willis anatomy strongly influences stroke patterns and outcomes. Poor collateralisation is associated with larger infarct cores and worse prognosis in large vessel occlusion. In aneurysm disease, branching points within the circle are exposed to high shear stress, explaining common aneurysm locations.
- ACom aneurysms → common cause of subarachnoid haemorrhage
- Variant anatomy alters stroke distribution
- Collateral status predicts thrombectomy outcomes
🧬 Developmental Basis
The Circle of Willis reflects embryological vascular development, where early carotid dominance gradually shifts toward vertebrobasilar supply. Incomplete regression or persistence of embryonic vessels explains many adult variants. This developmental perspective helps make variants logical rather than “anatomical trivia”.
🩺 Teaching Pearl
Never assume the Circle of Willis is complete. If infarcts cross arterial territories or symptoms do not fit a classic pattern, think variants. Understanding collateral flow turns vascular neurology from memorisation into physiology.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery