
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Breast
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
The breast (mammary gland) is a modified skin gland composed of glandular tissue, adipose (fat), and fibrous stroma, lying superficial to the pectoral fascia. Its core physiological role is lactation, but it also has major importance in sexual function, body image, and clinical medicine (especially benign disease and cancer). Breast structure is hormonally responsive across life stages-puberty, menstrual cycles, pregnancy, lactation, and menopause-changing tissue composition and imaging appearance.
1) External Anatomy
- Skin and subcutaneous tissue
- The breast is covered by skin containing sweat and sebaceous glands.
- The subcutaneous layer contains variable adipose tissue, which largely determines breast size and contour.
- Inframammary fold marks the inferior boundary; a key surgical landmark.
- Nipple–areola complex
- Nipple: contains smooth muscle → erection with cold, touch, and autonomic stimulation; multiple duct openings are present.
- Areola: pigmented skin around nipple; contains Montgomery glands (sebaceous glands) that lubricate and protect during breastfeeding.
- Clinical: new unilateral nipple inversion, eczema-like changes, or blood-stained discharge require assessment.
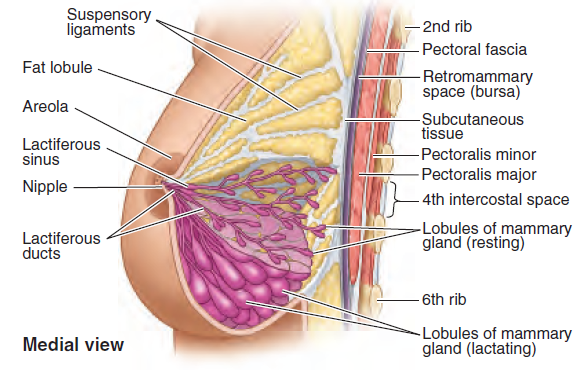
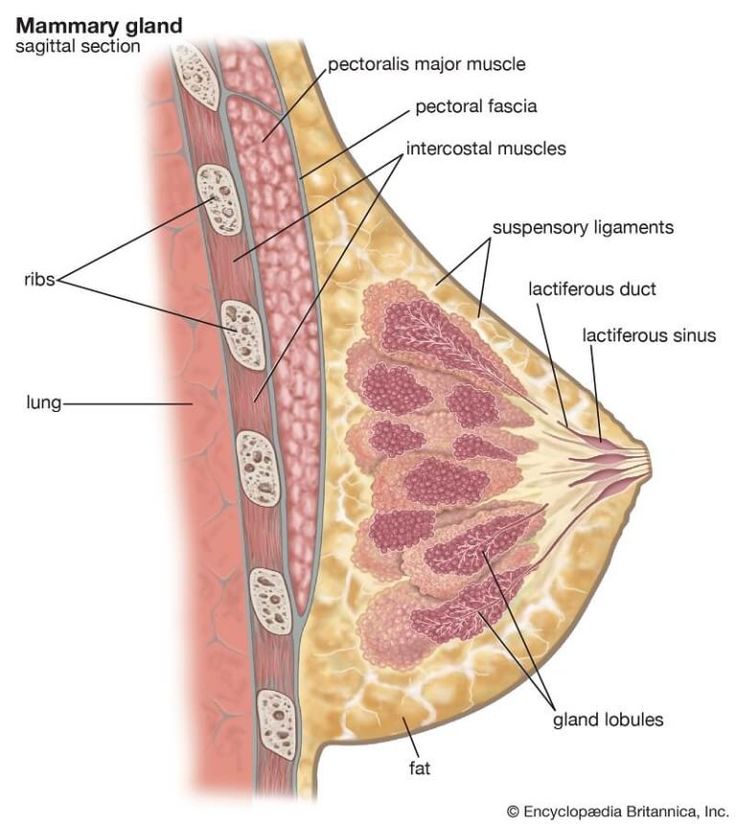
2) Internal Anatomy (Glandular + Stromal)
Internally, the breast is organised into lobes that drain via ducts to the nipple. Milk is produced in alveoli within lobules. Support comes from fibrous connective tissue (including Cooper’s ligaments) and the deep fascial plane over pectoralis major.
- Lobes and lobules
- Typically 15–20 lobes arranged radially around the nipple (anatomical variability is common).
- Each lobe is subdivided into lobules containing clusters of alveoli (milk-producing units).
- Alveolar cells secrete milk; surrounding myoepithelial cells contract to eject milk into ducts.
- Ductal system
- Lobules drain into lactiferous ducts that converge towards the nipple.
- Ducts are lined by epithelium supported by myoepithelial cells (important in pathology: many cancers arise from ductal/lobular epithelium).
- Clinical: duct ectasia and intraductal papilloma can cause nipple discharge.
- Connective tissue and support
- Cooper’s ligaments: fibrous septa from dermis to deep fascia; maintain breast shape.
- Clinical: malignancy can tether Cooper’s ligaments → skin dimpling.
- The breast lies in a “loose” plane (retromammary space) over pectoral fascia → allows some mobility on chest wall.
- Axillary tail (Tail of Spence)
- Glandular tissue can extend superolaterally into the axilla-important in examination and imaging.
3) Relations and Surface Anatomy (Exam + Surgery)
- Deep relation: pectoralis major fascia (with contributions near serratus anterior).
- Typical extent: from 2nd to 6th ribs and from lateral border of sternum to mid-axillary line (variable).
- Quadrants: upper outer quadrant contains the greatest volume of glandular tissue (and is a common location for lesions).
4) Vascular Supply
- Arterial supply
- Internal thoracic (internal mammary) artery perforators (medial breast).
- Lateral thoracic artery (from axillary artery; lateral breast).
- Posterior intercostal arteries contributions.
- Venous drainage
- Superficial and deep veins drain to axillary and internal thoracic veins.
- Clinical: venous/lymphatic obstruction can contribute to skin oedema and “peau d’orange”.
5) Lymphatic Drainage (High-yield for Cancer Staging)
Lymphatic drainage is central to breast cancer staging and surgical planning. Most lymph drains to the axillary nodes, but a significant portion drains medially to parasternal (internal mammary) nodes, which explains some patterns of metastatic spread.
- Axillary lymph nodes (major route)
- Especially from lateral and upper outer breast (including axillary tail).
- Sentinel node mapping targets first-draining nodes for staging.
- Internal mammary (parasternal) nodes
- More prominent drainage from medial breast.
- Supraclavicular nodes
- Can be involved in advanced disease.
6) Innervation
- Sensory innervation: anterior and lateral cutaneous branches of intercostal nerves (classically T2–T6).
- Nipple: rich sensory supply (often T4 dermatome) and important for the neuroendocrine milk ejection reflex.
- Autonomic: sympathetic fibres to vessels and smooth muscle (nipple erection).
7) Physiology
🧬 A) Hormonal Regulation Across Life
- Puberty: oestrogen drives ductal growth; progesterone supports lobuloalveolar development; fat deposition shapes breast contour.
- Menstrual cycle: cyclical oestrogen/progesterone changes cause variable fullness and tenderness (often luteal phase).
- Pregnancy: major lobuloalveolar proliferation; ducts enlarge; vascularity increases; preparation for milk production.
- Menopause: glandular tissue involutes with relative increase in fat and fibrous tissue.
🍼 B) Lactation: Milk Production vs Milk Ejection
Lactation has two linked processes: milk synthesis (driven by prolactin) and milk ejection (driven by oxytocin). The nipple–areola complex is the sensory trigger: suckling activates afferent nerves → hypothalamus → pituitary hormonal response.
- Milk production (Prolactin):
- Prolactin from anterior pituitary stimulates alveolar epithelial cells to synthesise milk proteins (and supports lactose and lipid production).
- Dopamine normally inhibits prolactin; suckling reduces dopamine → increases prolactin release.
- Milk ejection (“let-down”) (Oxytocin):
- Oxytocin from posterior pituitary causes myoepithelial cell contraction around alveoli and ducts → milk is propelled to nipple.
- Stress and pain can blunt let-down (sympathetic tone can inhibit oxytocin reflex).
- Colostrum: early milk rich in immunoglobulins and protective factors, providing neonatal immune support.
🛡️ C) Protective and Immune Aspects
- Breast milk contains immunological factors (e.g., IgA) that protect infant mucosa.
- Mastitis can occur when milk stasis and duct obstruction facilitate bacterial entry (often via nipple trauma).
8) Embryology (Clinically Relevant)
- Breast develops from the mammary ridge (milk line) extending from axilla to groin.
- Clinical: accessory nipples (polythelia) or ectopic breast tissue can occur along the milk line (including axilla).
- At puberty, hormonal stimulation drives maturation of ducts and lobules.
9) Clinical Significance
- Breast cancer:
- Understanding ductal/lobular anatomy and lymphatic drainage underpins diagnosis, imaging interpretation, sentinel node biopsy, and surgical planning.
- Classic signs: painless lump, skin tethering/dimpling, nipple changes, lymphadenopathy.
- Benign disease:
- Fibroadenoma: common benign solid lump in younger patients.
- Breast cysts: fluid-filled lesions; can fluctuate with cycle.
- Mastitis/abscess: typically lactational; pain, erythema, fever; treat promptly to protect feeding and prevent abscess.
- Gynaecomastia (male breast): glandular proliferation related to hormonal imbalance or medications.
- Surgery and imaging:
- Quadrant anatomy, axillary tail, and vascular/lymphatic routes are central to lumpectomy/mastectomy approaches and radiological localisation.
✅ Conclusion
The breast is an integrated organ of ducts, lobules (alveoli), stroma, fat, and skin, supported by Cooper’s ligaments and supplied by internal thoracic, lateral thoracic, and intercostal vessels. Physiologically it is highly hormone-responsive: prolactin drives milk synthesis and oxytocin drives milk ejection, coordinated by nipple sensory input. Clinically, mastery of anatomy-especially lymphatic drainage and the nipple–areola complex-directly informs examination, imaging interpretation, and cancer staging/surgery.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery