
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Femoral Vein Cannulation
Related Subjects: Atropine |Acute Anaphylaxis |Basic Life Support |Advanced Life Support |Adrenaline/Epinephrine |Acute Hypotension |Cardiogenic shock |Distributive Shock |Hypovolaemic or Haemorrhagic Shock |Obstructive Shock |Septic Shock and Sepsis |Shock (General Assessment) |Toxic Shock Syndrome
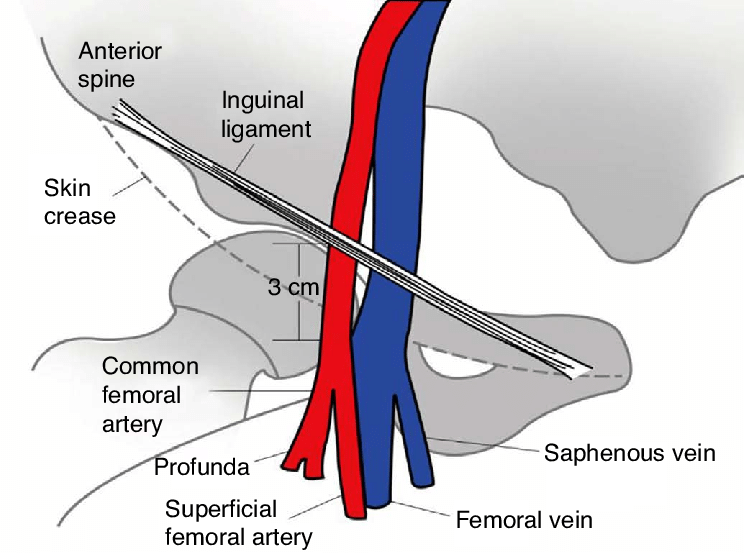
⚠️ Key Safety Notes: Always remain medial to the femoral arterial pulse to avoid arterial puncture. Ultrasound guidance significantly improves success rate and reduces complications (arterial puncture, attempts, infection risk).
🩺 Procedure Steps
- Patient Position: Supine, leg slightly externally rotated and abducted for optimal femoral triangle access.
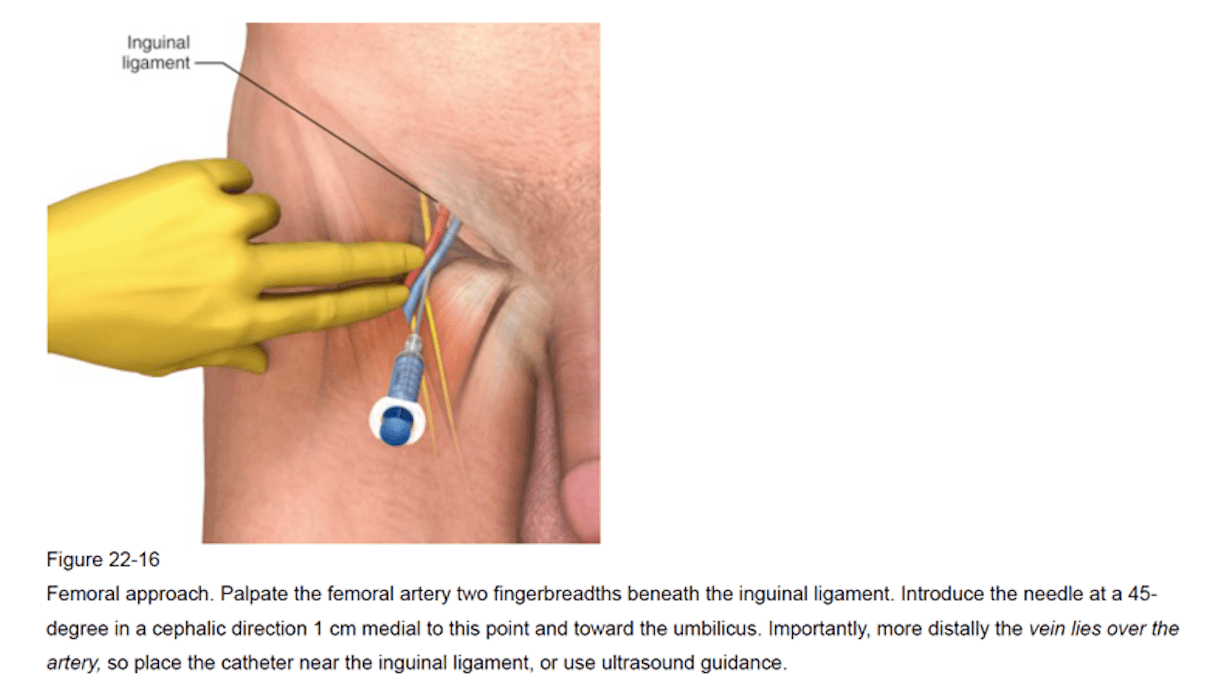
- Landmark: Femoral vein lies immediately medial to femoral artery (mnemonic: NAVY – Nerve, Artery, Vein, Y-fronts). Use real-time ultrasound rather than landmark/palpation alone (standard of care).
- Preparation: Full aseptic technique - chlorhexidine skin prep, maximal barrier drapes, sterile probe sheath, flushed ports, sterile gown/gloves.
- Local Anaesthetic: Infiltrate skin and subcutaneous tissue with 1% lidocaine (under US if possible).
- Needle Insertion: Insert 18G introducer needle at ~45° angle to skin while aspirating continuously. Confirm venous flashback (dark, non-pulsatile blood). Anchor needle securely.
- Guidewire: Advance J-tip guidewire smoothly through needle. Never force if resistance met (risk of vessel perforation or wire kinking).
- Needle Removal: Withdraw introducer needle while holding wire firmly in place.
- Skin Incision: Small nick with #11 scalpel blade to ease dilator passage (avoid cutting wire).
- Dilatation: Pass dilator over wire to form tract; remove dilator once tract created.
- Catheter Insertion: Advance central venous catheter over wire, always controlling the proximal end of the wire. Remove wire once catheter fully seated.
- Confirmation: Aspirate and flush all lumens (venous blood), secure with sutures/staples, apply occlusive sterile dressing.
- Disposal & Documentation: Dispose sharps immediately; document indication, technique, US findings, complications, and post-procedure CXR (if required for tip position).
⚠️ Complications & Management
- Common: Line-related infection (CLABSI), thromboembolism/DVT, arterial puncture (1–5% landmark, <1% US), haematoma (prolonged manual pressure in coagulopathy).
- Rare: Arteriovenous fistula, pseudoaneurysm, retroperitoneal haemorrhage, vessel perforation, nerve injury.
- Arterial Puncture: Withdraw needle, apply firm pressure ≥10–15 min; monitor for expanding haematoma or distal ischaemia; consider surgical consult if persistent.
- Haematoma: Usually conservative management; ongoing bleeding or compartment syndrome → urgent surgical review.
📚 References
- NEJM: Femoral Vein Cannulation Technique (classic article/video series)
- TeachMeAnatomy / Elsevier / Cardiac Interventions Today (US-guided access tutorials)
- Current guidelines: CDC, SHEA, ASE (ultrasound mandatory for femoral CVC in most settings)
Clinical Pearl:
Always confirm venous placement (aspiration of dark non-pulsatile blood + US visualization) before advancing wire/catheter or using the line.
In OSCEs/MCQs, examiners expect emphasis on: real-time ultrasound guidance, medial-to-artery approach, guidewire safety ("never force"), strict asepsis, and prompt complication recognition.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery