
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Fever Pyrexia of unknown origin (FUO PUO)
Related Subjects: | Fever in a Traveller | Malaria Falciparum | Malaria Non Falciparum | Viral Haemorrhagic Fevers (VHF) | Lassa Fever | Dengue | Marburg Virus Disease | AIDS/HIV | Yellow Fever | Ebola Virus | Leptospirosis | Crimean-Congo Haemorrhagic Fever | African Trypanosomiasis (Sleeping Sickness) | American Trypanosomiasis (Chagas Disease) | Incubation Periods | Notifiable Diseases UK
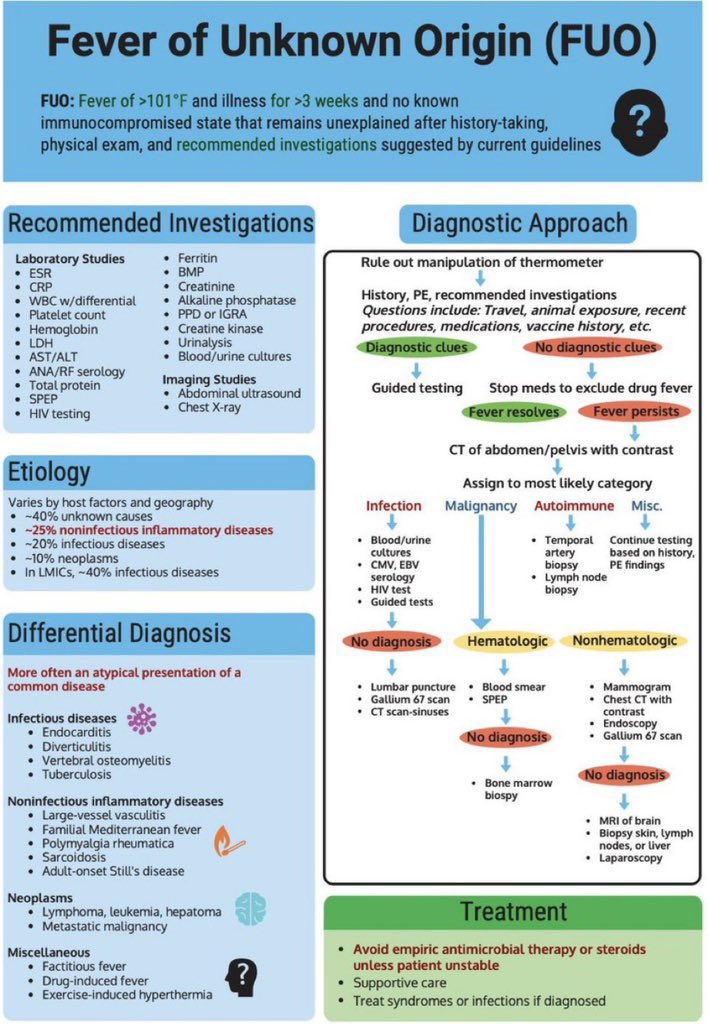
🌡️ Key Point: FUO requires multiple expert opinions because causes are broad, and not all prolonged fevers are infectious. Current definition: PUO is defined as fever >38.3 °C on several occasions, lasting >3 weeks, with no diagnosis after 1 week of inpatient investigation. Any pyrogen (microbial toxin, cytokine, necrotic material) can trigger fever.
📖 About
- Original (Petersdorf & Beeson, 1960s): Temp >38.3 °C for >3 weeks with no diagnosis after 1 week of inpatient work-up (pre-CT/MRI era).
- Current: Fever >2 weeks with no diagnosis despite detailed investigations. Fever = cytokines/interferons reset hypothalamic set point. 🚨 Fever may be reduced or absent in elderly, steroid-treated, or immunocompromised patients.
🧾 Definitions
- Current: >2 weeks, unexplained after thorough testing.
- Original: >38 °C, >3 weeks, unexplained after 1 week hospital investigations.
🩺 Differential Diagnoses
- Infections: TB, endocarditis, urinary/resp tract infections.
- Abscesses: Pelvic, renal, epidural, subdiaphragmatic.
- Tropical/Parasitic: Malaria, amoebiasis, leishmaniasis, trypanosomiasis.
- Other infections: EBV/CMV, brucellosis, HIV, Lyme, Whipple’s, rickettsiae.
- Rheumatological: GCA, PMR, SLE, Still’s, vasculitides.
- Genetic: Familial Mediterranean Fever.
- Malignancy: Lymphoma, leukaemia, renal cell carcinoma, solid tumours.
- Other: Drug fever, atrial myxoma, thyrotoxicosis.
🔑 Key Clinical Approaches
- 🧳 History: travel, drug use (esp. IV), occupational & sexual exposures.
- 👀 Exam: skin, oral/dental, lymph nodes, rectal/pelvic where indicated.
- 📸 Imaging: chest X-ray, ultrasound, CT/MRI → hidden abscess/malignancy.
- 🔁 Re-evaluate: repeat history/exam frequently; new clues often evolve.
- 🤝 Seek early specialist input: rheumatology, haematology, microbiology, cardiology.
🔬 Investigations
- Basic labs: FBC, ESR/CRP, LFTs, U&Es, TFTs.
- Serology: EBV, CMV, HIV, Bartonella, Toxoplasma, Brucella, Lyme, Q fever.
- Microbiology: Blood, urine, stool cultures (≥3 sets); wound swabs if relevant.
- Imaging: CXR, abdo/pelvic US, CT, MRI.
- Specialised: Echocardiogram (endocarditis/myxoma), malaria films (×3), autoimmune panels (ANA, ANCA, RF).
- Biopsy: Liver (TB, lymphoma, granulomas), bone marrow (malignancy, leishmaniasis, TB), temporal artery (>50yrs, rule out GCA).
- FDG PET/CT: Has increasingly important diagnostic yield, especially where inflammatory, malignant, or occult infective foci are suspected. That does not mean every patient needs PET-CT, only that it is more contemporary than foregrounding labelled white-cell scans.
📊 Causes of FUO
| Category | Examples / Notes |
|---|---|
| 🦠 Common Infections (30–40%) | UTI, chest infections, endocarditis. Take blood cultures before antibiotics. |
| 🦟 Malaria | Travel history vital. Falciparum malaria = rapidly fatal. Do thick & thin films. |
| 🧫 Tuberculosis | Miliary/extrapulmonary. May need CXR, IGRA, biopsy. |
| 💥 Abscess | Splenic, perirenal, pelvic, spinal. Requires CT/US/MRI for localisation. |
| 🧬 Other Infections | HIV, osteomyelitis, typhoid, brucellosis, Lyme, EBV, CMV, Bartonella, toxoplasmosis. |
| 🎗️ Malignancy (~20%) | Lymphoma, leukaemia, renal cell carcinoma. Often ↑ESR/LDH. |
| 🔥 Inflammatory (10–20%) | GCA, Still’s, SLE, vasculitis, RA. Very high ESR in GCA. |
| ⚖️ Miscellaneous | Atrial myxoma, sarcoidosis, Crohn’s, FMF, occult haematoma, thyrotoxicosis. |
| ❓ Idiopathic | No diagnosis despite extensive work-up. |
| 💊 Drugs | Drug-induced fever; thorough med history crucial. |
| 🕵️ Factitious | Deliberate fever. Normal ESR/CRP. Consider when the pattern is inconsistent and inflammatory markers remain normal, but diagnose cautiously after excluding organic disease |
🧑⚕️ Management Principles
- 🚫 Avoid “blind” antibiotics when appropriate- they obscure cultures & mask clues. See below for qualifier
- ✅ Re-evaluate regularly; revisit history & exam with fresh eyes.
- 🤝 Discuss with seniors & specialists early (multidisciplinary approach).
- 📅 Stable outpatients: follow up carefully; unstable patients → urgent admission.
- 💊 Suspend unnecessary meds to rule out drug fever.
Avoid “blind antibiotics” is good advice for classical FUO, but it needs one safety qualifier. In a genuinely unstable patient, or where there is concern for sepsis, neutropenic sepsis, or another time-critical syndrome, treatment should not be withheld just to preserve diagnostic purity. That distinction is important clinically and prevents the note from being misread as “never start empiric treatment.”
Teaching Commentary 🌡️
PUO is defined as fever >38.3 °C on several occasions, lasting >3 weeks, with no diagnosis after 1 week of inpatient investigation. Causes fall into 4 groups: 1. Infections (TB, endocarditis, abscesses). 2. Malignancies (lymphoma, leukaemia, renal carcinoma). 3. Autoimmune/Inflammatory (GCA, Still’s disease, vasculitis, SLE). 4. Miscellaneous (drug fever, thyroiditis, sarcoidosis). Approach: repeat history/exam, serial blood cultures, imaging (CXR, CT, PET-CT), autoimmune panel, consider biopsy. Always review medications. Management is cause-specific - avoid empirical steroids/antibiotics until diagnosis unless patient is acutely unstable.
Cases - Pyrexia of Unknown Origin (PUO / FUO)
- Case 1 - Infective (Tuberculosis): A 35-year-old man presents with 6 weeks of intermittent fever, night sweats, and weight loss. No cough. CXR: miliary mottling. ESR raised, Quantiferon positive. Diagnosis: Disseminated tuberculosis. Management: Anti-TB therapy (RIPE regimen), prolonged course; notify public health.
- Case 2 - Infective (Endocarditis): A 52-year-old man with a prosthetic mitral valve presents with 5 weeks of low-grade fever, sweats, and weight loss. Exam: new murmur, splinter haemorrhages. Blood cultures: *Streptococcus viridans*. Echo: vegetation. Diagnosis: Infective endocarditis. Management: Prolonged IV antibiotics ± surgery if refractory or valve destruction.
- Case 3 - Malignancy (Lymphoma): A 42-year-old woman has 2 months of fever, drenching night sweats, and weight loss. Exam: cervical lymphadenopathy, splenomegaly. LDH high. Node biopsy: Reed–Sternberg cells. Diagnosis: Hodgkin lymphoma. Management: Staging and chemotherapy (ABVD regimen).
- Case 4 - Autoimmune (Adult-Onset Still’s Disease): A 28-year-old woman has daily spiking fevers, arthralgia, and a salmon-pink rash. Labs: neutrophilia, high ferritin, negative ANA/RF. Diagnosis: Adult-onset Still’s disease. Management: NSAIDs or corticosteroids; consider biologics if refractory.
- Case 5 - Autoimmune (Giant Cell Arteritis): A 70-year-old woman presents with fever, weight loss, new headache, and scalp tenderness. ESR 110 mm/hr. Temporal artery tender and thickened. Diagnosis: Temporal arteritis presenting as PUO. Management: High-dose corticosteroids immediately; confirm with temporal artery biopsy.
- Case 6 - Miscellaneous (Drug Fever): A 65-year-old man on long-term antibiotics for osteomyelitis develops persistent fever without focus. All cultures negative. Fevers stop 48 hours after stopping beta-lactam therapy. Diagnosis: Drug-induced PUO. Management: Stop culprit drug; supportive care.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery