Transverse myelitis
Related Subjects:
|Neurological History taking
|Motor Neuron Disease (MND-ALS)
|Miller-Fisher syndrome
|Guillain Barre Syndrome
|Multifocal Motor Neuropathy with Conduction block
|Inclusion Body Myositis
|Multiple Sclerosis (MS) Demyelination
|Transverse myelitis
|Acute Disseminated Encephalomyelitis
|Cervical spondylosis
|Spinal Cord Anatomy
|Acute Disc Prolapse
|Spinal Cord Compression
|Spinal Cord Haematoma
|Foix-Alajouanine syndrome
|Cauda Equina
|Conus Medullaris syndrome
|Anterior Spinal Cord syndrome
|Central Spinal Cord syndrome
|Brown-Sequard Spinal Cord syndrome
|Vitamin B12 deficiency
|Myelopathy
|Spinal Cord Arteriovenous Malformations
📖 About
- Transverse Myelitis = inflammatory disorder of the spinal cord, affecting grey + white matter and producing motor, sensory, and autonomic dysfunction.
- 🧍♂️ Bimodal distribution: most common in ages 10–20 and >40 years.
- Symptoms vary depending on cord level and whether the lesion is partial or complete.
🔬 Aetiology
- Involves both grey and white matter → wide range of deficits.
- Lesion may be partial (one side/segment) or complete (whole cord cross-section).
🧾 Causes
- ⚡ Autoimmune: MS, ADEM, Neuromyelitis Optica (NMOSD).
- 🌐 Systemic Autoimmune Disease: SLE, Sjögren’s, vasculitis, sarcoid.
- 🦠 Infections: Viral (HIV, EBV, Coxsackie, Zika), Bacterial (Mycoplasma), rare fungal/parasitic.
- 🎗 Paraneoplastic: esp. small-cell lung cancer.
- 💉 Post-vaccination: Rare, causality debated.
⚡ Risk Factors
- Recent infection.
- History of autoimmune disease.
- Genetic predisposition to demyelination.
- Occasional link with recent immunisation.
🩺 Clinical Presentation
- ⏱ Onset: Rapid (hours–days) or subacute (weeks).
- 🌡 Initial: Fever, back pain, myalgia, “band-like” tightness around trunk.
- ⚡ Pain: Often sharp, radiating along dermatomes.
- 💪 Weakness: Spastic paraparesis or quadriparesis.
- 🧊 Sensory loss: Numbness, tingling, loss of pain/temp below level.
- 🚽 Autonomic: Urinary retention, incontinence, constipation.
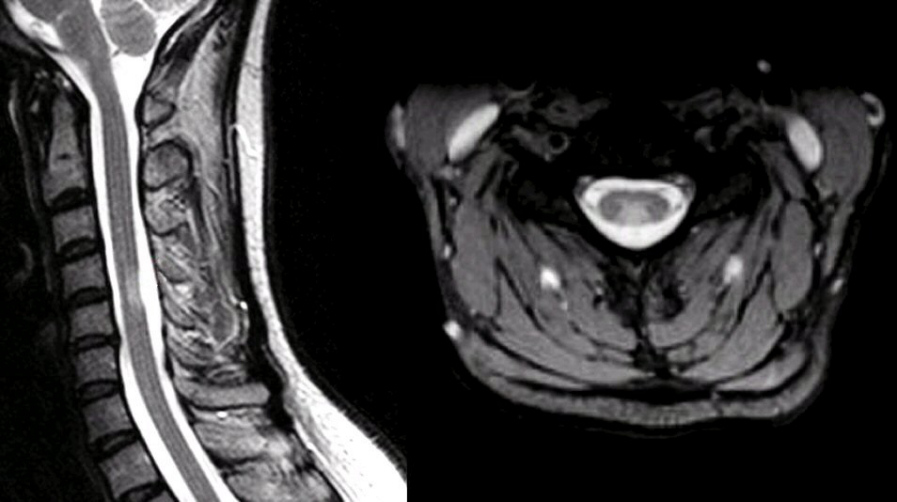
🖼 MRI
🚨 Red Flags
- Sudden severe progression of weakness.
- Respiratory involvement → cervical/high thoracic lesions (can cause ventilatory failure).
- Systemic “B symptoms”: fever, night sweats, weight loss (consider infection/malignancy).
🧪 Investigations
- 🖥 MRI + contrast: Exclude compression, shows T2 hyperintensities spanning ≥3 vertebral segments in NMOSD.
- 💉 CSF: Pleocytosis, raised protein, oligoclonal bands (MS).
- 🧬 Bloods: ANA, ANCA, HIV, EBV, syphilis, aquaporin-4 antibodies (NMOSD).
- ⚡ Evoked Potentials: Detect conduction block in demyelinating disease.
🔍 Differential Diagnosis
- Spinal cord compression (tumour, disc, abscess).
- Multiple sclerosis.
- Spinal cord infarction.
- Neuromyelitis optica spectrum disorder (NMOSD).
- SLE/Sjögren’s-related myelopathy.
💊 Management
- Acute Phase:
- 💉 IV methylprednisolone (3–5 days) → dampens inflammation, improves recovery.
- 🩸 Plasma exchange (PLEX) → for steroid-refractory cases, esp. NMOSD.
- 💉 IVIG → alternative in autoimmune or post-infectious causes.
- Supportive Care: Pain relief, catheterisation, physio, OT.
- Long-term:
- Disease-modifying therapy if underlying MS/NMOSD.
- Immunosuppression in SLE, Sjögren’s, sarcoid.
- Regular rehab to optimise function.
📈 Prognosis
- Variable → some recover fully, others left with deficits.
- Better outcomes with early steroids & limited lesion length.
- NMOSD-related transverse myelitis often severe, relapsing, long cord lesions (“longitudinally extensive TM”).
📝 Exam Pearl: TM = motor + sensory + autonomic dysfunction.
Red flag = rapid onset with preserved dorsal column sensation → think infarction instead.
Always exclude compressive lesions on MRI before labelling “transverse myelitis.”
