
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Bell's Palsy (Facial nerve palsy)
Related Subjects: |Bell's (Facial Nerve) palsy |Ramsay Hunt syndrome |Facial nerve anatomy
😮 Bell's Palsy is an idiopathic, acute, unilateral lower motor neuron (LMN) facial nerve palsy. ⚡ Develops rapidly (within 72 hours) and does not progress further after that. ❌ A gradually progressive palsy is not Bell’s Palsy. Ear and facial pain are common and do not necessarily imply middle ear disease.
📌 About
- Often mistaken for stroke, but Bell’s Palsy involves the entire face including the forehead (LMN lesion).
- Named after Sir Charles Bell (1774–1842).
- Incidence: 15–30 per 100,000 people annually; men and women equally affected.
🧠 Anatomy of CN VII
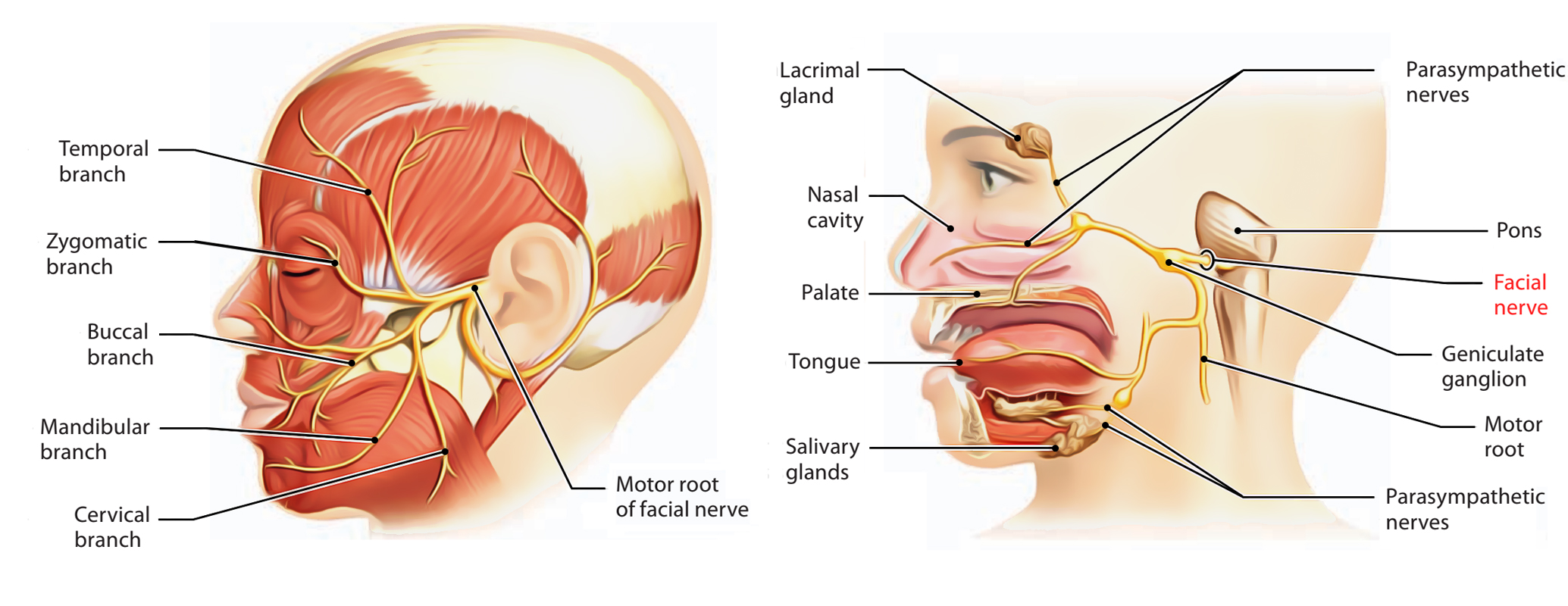
- Mixed cranial nerve (motor > sensory > parasympathetic).
- Courses through the temporal bone in a narrow canal → vulnerable to inflammation and compression.
🦠 Aetiology
- Mostly idiopathic, but thought to be post-viral (HSV, VZV).
- When caused by VZV (with vesicles) → Ramsay Hunt Syndrome.
🤒 Clinical Features
- Rapid unilateral facial weakness, maximal within hours to days.
- Ear pain on affected side.
- Weakness involves forehead, eye, and mouth (LMN pattern).
- Other features: altered taste (ant. 2/3 tongue), hyperacusis, reduced tear production, impaired corneal reflex.
- Bell’s sign: Eye rolls up/out when attempting closure.
- Look carefully for vesicles (Ramsay Hunt) or other CN palsies (e.g. VI nerve with pontine lesions).
🚫 Key Exclusions
- Other neurological deficits.
- Abnormal ear/throat exam (vesicles, tumours, OM).
- Neck or parotid masses.
- Consider Lyme disease, sarcoid, skull base pathology if atypical.
🧑⚕️ Examination Notes
- VII is primarily motor, but patients may report “numbness” despite intact sensation.
- Tests:
- Ask to smile/show teeth → affected side droops.
- Ask to close eyes → incomplete closure, Bell’s sign visible.
- Forehead wrinkling reduced on affected side.
🦠 HIV: Facial nerve palsy is ~100× more common in HIV patients than immunocompetent patients.
🩺 Differentials
- Parotid tumour (often malignant).
- Lyme disease (bilateral LMN VII, rash/joint pain).
- Sarcoidosis (Heerfordt’s syndrome, hilar lymphadenopathy).
- Guillain-Barré (bilateral LMN VII + limb paraesthesia).
- Stroke: UMN → forehead spared.
- Pontine stroke: LMN VII + VI palsy ± contralateral weakness.
🔎 Investigations
- Primarily clinical diagnosis.
- Bloods: FBC, U&E, glucose, ESR, TFTs if atypical.
- MRI: Consider if atypical (pons lesion, tumour, geniculate ganglion enhancement).
- Nerve conduction/EMG: Occasionally useful to grade nerve damage.
📊 House–Brackmann Classification
- I – Normal
- II – Mild dysfunction (minimal asymmetry)
- III – Moderate dysfunction (incomplete smile, but eye closure possible)
- IV – Severe dysfunction (obvious weakness, incomplete eye closure)
- V – Minimal movement
- VI – Complete paralysis
⚠️ Complications
- Residual facial weakness.
- Synkinesis (involuntary movements, e.g. eye closes when smiling).
- Hearing loss or neuropathic pain.
💊 Management
- Steroids: If onset <72h, Prednisolone 60 mg daily (taper over 10 days). → Increases recovery rate (81.6% → 94.4%). Avoid/adjust in pregnancy, diabetes, glaucoma, ulcers, elderly with osteoporosis.
- Antivirals: Only if vesicles present (Ramsay Hunt) → Aciclovir 800 mg 5×/day ×7 days.
- Eye care: Artificial tears, Lacrilube at night, tape/patch if cornea exposed.
- Recovery: Usually within 3–6 months.
📞 Referral
- Uncertain diagnosis, recurrent, or bilateral cases.
- Urgent ophthalmology if cornea exposed.
- ENT if no improvement at 1 month, or persistent weakness >6–9 months (may need plastics).
📉 Poor Prognostic Factors
- Complete palsy with no recovery by 3 weeks.
- Age >60, severe pain, Ramsay Hunt, diabetes, hypertension, pregnancy.
- Severe nerve degeneration on EMG.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery