Castleman's disease
🦠 HHV-8 is the well-established cause of HHV-8-associated Multicentric Castleman Disease (MCD), accounting for ~50% of MCD cases.
📖 About
- Castleman disease first described in 1954.
- A rare lymphoproliferative disorder affecting lymph nodes and surrounding tissues.
- Two main forms: Unicentric CD (UCD) and Multicentric CD (MCD).
- Also called angiofollicular lymph node hyperplasia or benign giant lymph node hyperplasia.
🧬 Aetiology
- Exact cause unknown.
- Some patients have HIV and/or HHV-8 infection.
- UCD ➝ IL-6 driven.
MCD ➝ IL-6 + HHV-8 involvement.
- IL-6 overproduction drives inflammation and acute-phase response.
📌 Clinical Types
- Unicentric CD (UCD): Localised to one lymph node region.
- Multicentric CD (MCD): Systemic, affecting multiple lymph nodes + other organs.
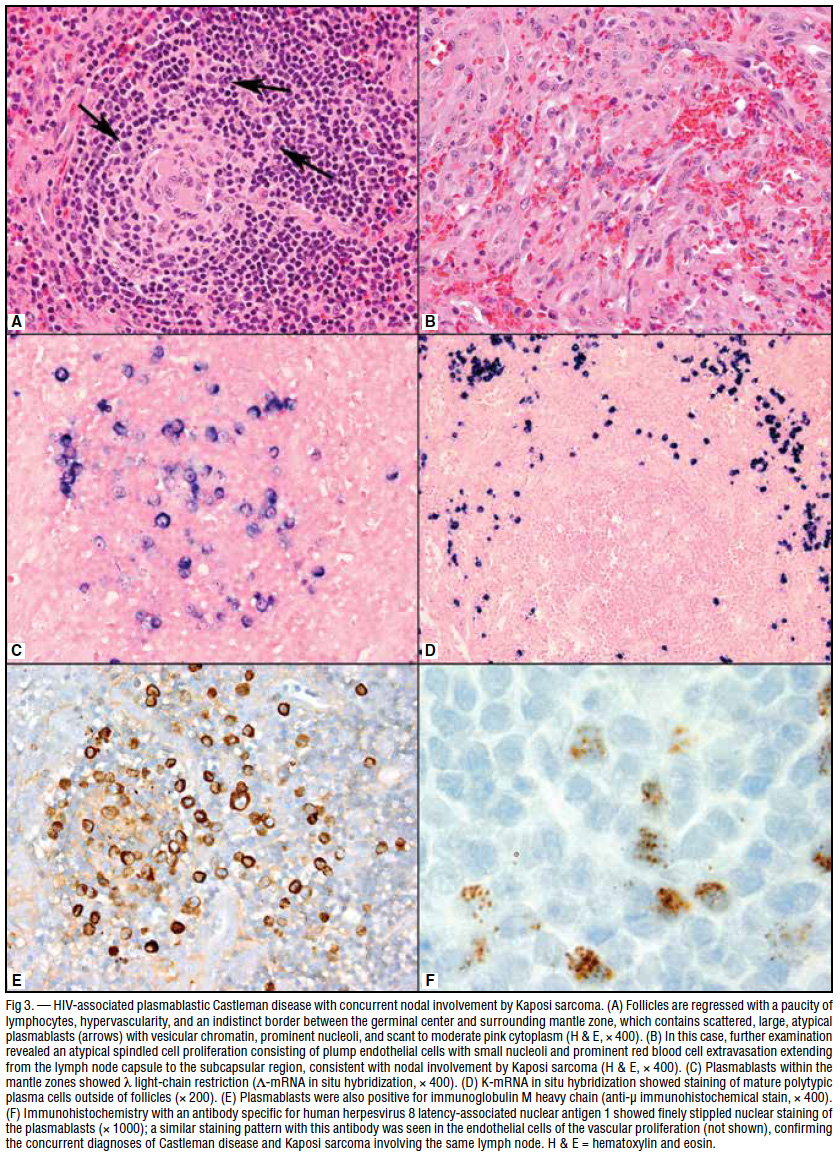
🔬 Pathological Types
- Hyaline-Vascular Type: ~90% cases; follicles with hyalinised vessels + concentric lymphocytes + vascular stroma.
- Plasma Cell Type: Dense sheets of plasma cells in interfollicular tissue, minimal vascular stroma.
🧩 Associated Conditions
- Large B-cell lymphoma
- POEMS syndrome
- Follicular dendritic cell sarcoma
- Paraneoplastic pemphigus
- Kaposi sarcoma (esp. HHV-8 MCD)
- Eruptive cherry haemangiomas / violaceous papules
- Lymphocytic interstitial pneumonitis
🩺 Clinical Presentation
- B symptoms: Fever 🌡️, night sweats 😓, weight loss ⚖️.
- UCD: Dx mean age ~34, F>M. Painless lymphadenopathy in chest (30%), neck (23%), abdomen (20%), retroperitoneum (17%). May have B symptoms.
- MCD: Age ~50s (younger in HIV/HHV-8), M>F. Findings:
- Generalised lymphadenopathy
- Hepatosplenomegaly
- Fluid retention ➝ oedema, effusions, ascites
- B symptoms
🧪 Investigations
- Bloods: Anaemia, ↑ CRP/ESR, thrombocytosis or thrombocytopenia.
- Biochemistry: Hypergammaglobulinaemia, hypoalbuminaemia, renal impairment.
- Cytokines: ↑ IL-6, IL-10.
- Serology: HIV + HHV-8 testing; HHV-8 DNA load correlates with symptoms + relapse.
- Imaging (CT/MRI): Enlarged nodes, hepatosplenomegaly, systemic spread.
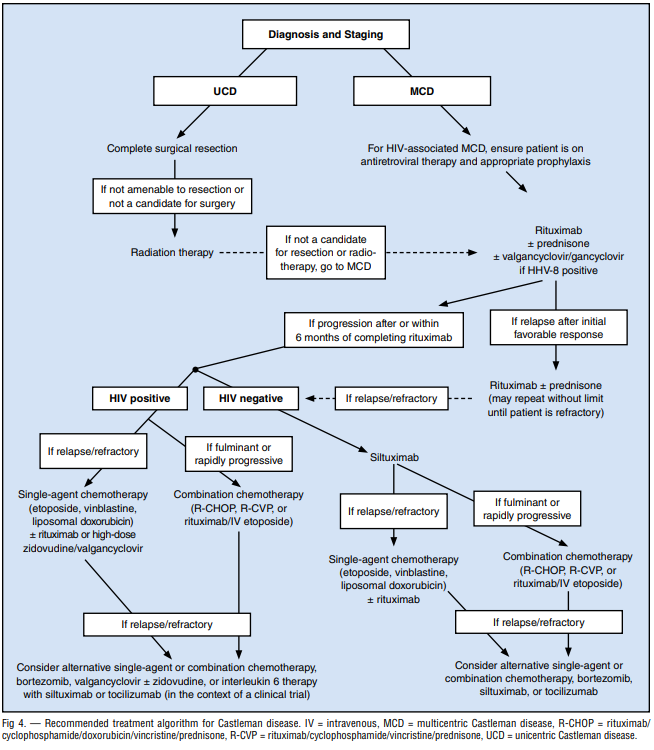
💊 Management
- Unicentric CD:
- Usually hyaline-vascular type.
- Curable with surgical resection.
- Radiotherapy is an alternative with high response rates.
- Multicentric CD:
- First-line: Rituximab (esp. HHV-8+). Add HAART in HIV cases.
- IL-6 Blockade: Siltuximab (FDA-approved for HIV-/HHV-8- MCD), Tocilizumab also used.
- Cytotoxic Chemotherapy: Etoposide, vinblastine, cyclophosphamide, cladribine, chlorambucil, liposomal doxorubicin.
- Immunotherapy: Rituximab + steroids (Prednisone 1 mg/kg) until controlled, then taper.
- Supportive Care: Manage infections, malignancies, paraneoplastic syndromes.
📊 Algorithm
📚 References
