Related Subjects:
|Herpes Varicella-Zoster (Shingles) Infection
|Chickenpox Varicella Infection
|Varicella Cerebral Vasculopathy
|Herpes Viruses
|Herpes Zoster Ophthalmicus (HZO) Shingles
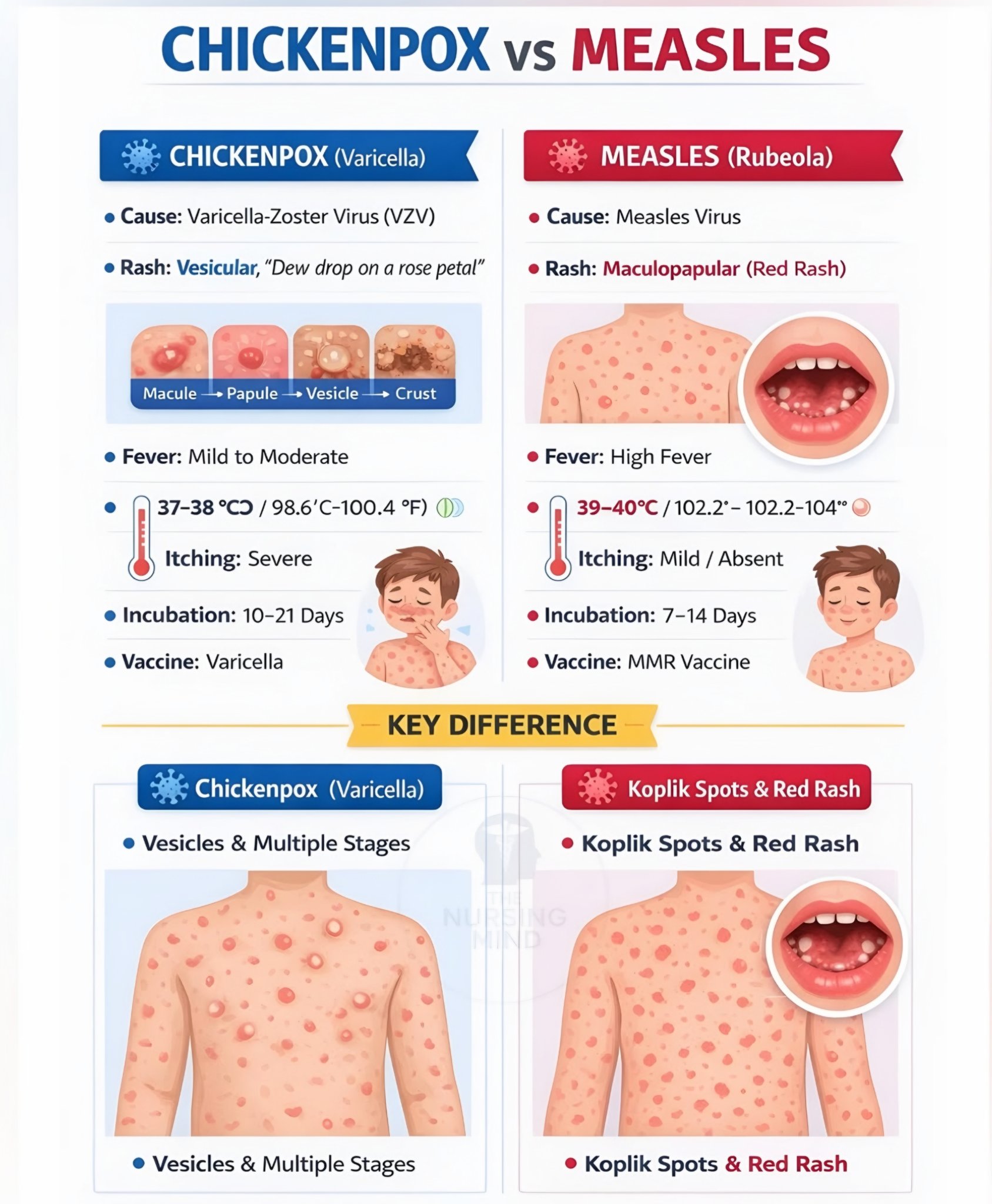
🦠 Varicella-zoster virus (VZV) causes chickenpox (varicella) as the primary infection and later may reactivate as shingles (herpes zoster). Chickenpox is usually mild in healthy children, but it can be severe in adults, pregnant women, neonates, and immunocompromised people. In England, routine childhood protection has changed: from January 2026, the NHS introduced the MMRV vaccine at 12 months and 18 months.
ℹ️ About
- VZV is a highly contagious herpesvirus.
- Primary infection causes chickenpox; after recovery, the virus remains latent in dorsal root and cranial nerve ganglia.
- Later reactivation causes shingles.
- Exposure to chickenpox can cause chickenpox in susceptible contacts; exposure to shingles can also cause chickenpox in a non-immune person if they have direct contact with lesions.
- Adults usually have more severe disease than children and are at higher risk of complications.
🧬 Transmission and infectivity
- Spread occurs by respiratory droplets, airborne spread, and direct contact with vesicle fluid.
- Secondary attack rates in susceptible household contacts are very high.
- The usual incubation period is about 10–21 days.
- People with chickenpox are infectious from about 1–2 days before rash onset until all lesions have crusted over.
- People with shingles are infectious while vesicles are present, particularly if lesions are uncovered.


🩺 Clinical features
- Prodrome may include fever, malaise, headache, and myalgia.
- The rash is classically itchy and appears in crops.
- Lesions are seen at different stages at the same time: macules → papules → vesicles → crusts.
- Typical lesions are often described as “dew drops on a rose petal”.
- The rash usually starts on the trunk, scalp, and face, then spreads.
- Mucosal lesions may occur.
- Immunocompromised patients may develop more extensive, prolonged, or disseminated disease.
⚠️ Complications
- Bacterial superinfection of skin lesions.
- Varicella pneumonia, especially in adults, smokers, and pregnancy.
- Neurological complications: cerebellitis, encephalitis, meningitis.
- Dehydration, especially in children with poor oral intake.
- Less commonly: hepatitis, myocarditis, nephritis, thrombocytopenia.
- Severe disseminated disease may occur in immunocompromised people and neonates.
👶 Children
- In healthy children, chickenpox is usually self-limiting.
- Symptomatic treatment and hydration are usually sufficient.
- Avoid ibuprofen and other NSAIDs if possible in chickenpox because of an association with severe skin and soft tissue complications.
- Avoid aspirin in children because of the risk of Reye’s syndrome.
🧪 Investigations
- Diagnosis is usually clinical.
- If uncertain, PCR from vesicle fluid is the most useful confirmatory test.
- VZV IgG serology can be used to check immunity after exposure in selected groups, especially pregnancy.
- Blood tests and imaging are guided by complications, for example hypoxia, pneumonia, encephalitis, or sepsis.
💊 General management
- Encourage fluids and avoid dehydration.
- Use paracetamol for fever or discomfort.
- Itch may be eased with cooling measures, loose clothing, emollients, or an age-appropriate antihistamine if needed.
- Children should usually stay away from school or nursery until all spots have crusted over.
- Avoid contact with pregnant women, immunocompromised people, and newborn babies until no longer infectious.
💉 Antiviral treatment
- Antiviral treatment is not routinely needed for otherwise healthy young children with uncomplicated chickenpox.
- Consider oral aciclovir in adults or adolescents, especially if started within 24 hours of rash onset.
- Seek specialist or urgent secondary-care advice for immunocompromised patients, pregnant women, neonates, or anyone with severe complications.
- Intravenous aciclovir is used for severe disease such as pneumonia, encephalitis, disseminated infection, or severe immunocompromise.
🤰 Chickenpox in pregnancy
- Chickenpox in pregnancy can be serious for the mother, with increased risk of varicella pneumonia and severe disease.
- Maternal infection in early or mid-pregnancy carries a small risk of congenital varicella syndrome.
- Infection around the time of delivery can cause neonatal varicella, which may be severe.
- Pregnant women with exposure or suspected chickenpox need urgent assessment.
- Those with a clear history of previous chickenpox or shingles usually do not need testing or post-exposure prophylaxis unless immunosuppressed.
- If immunity is uncertain, urgent VZV IgG testing is often used to guide management.
🛡️ Post-exposure prophylaxis (PEP)
- PEP is aimed at people at high risk of severe disease, especially:
- pregnant women without confirmed immunity,
- immunocompromised people,
- certain neonates and young infants.
- Current UKHSA guidance recommends oral antiviral PEP for many at-risk contacts.
- Varicella-zoster immunoglobulin (VZIG) is mainly reserved for specific neonatal situations and selected high-risk cases, rather than being the default option for everyone.
- Pregnant contacts from 20 weeks’ gestation who are susceptible are offered antiviral PEP under UKHSA guidance.
🤰 Treatment in pregnancy
- Pregnant women with chickenpox should seek urgent GP, maternity, or obstetric advice.
- Oral aciclovir can be considered, particularly if started early and especially after 20 weeks’ gestation.
- IV aciclovir is indicated for severe disease such as pneumonia, encephalitis, or significant maternal systemic illness.
- Hospital assessment is needed if there is breathlessness, chest pain, neurological symptoms, extensive rash, or significant systemic illness.
👶 Neonates and immunocompromised people
- Neonates exposed around the time of maternal infection are at particular risk of severe disease.
- Immunocompromised people may have atypical, disseminated, or prolonged infection.
- These groups need same-day specialist advice about testing, prophylaxis, and treatment.
💉 Vaccination
- From 1 January 2026, the NHS routine childhood schedule includes MMRV vaccination at 12 months and 18 months.
- The routine schedule has replaced the previous MMR-only doses at those ages for eligible children.
- Some older children are also eligible for catch-up under the national implementation programme.
- Before 2026, varicella vaccination in the UK was mainly limited to selected contacts of vulnerable individuals; this has now changed.
🚨 Red flags
- Pregnancy
- Immunocompromise
- Neonate or very young infant
- Breathlessness, cough, or hypoxia
- Confusion, ataxia, seizures, or severe headache
- Rapidly progressive rash, haemorrhagic lesions, or severe secondary bacterial infection
- Poor oral intake or dehydration
💡 Clinical pearl: Chickenpox is often mild in children, but adults, pregnant women, neonates, and immunocompromised patients are the key high-risk groups. In pregnancy, always ask: Was there definite past chickenpox or shingles? If not, check immunity urgently and seek same-day advice about prophylaxis.
📚 References
