
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Modified Valsalva
- Indications: The modified Valsalva manoeuvre is primarily used as a non-invasive treatment for supraventricular tachycardia (SVT), specifically paroxysmal SVT (PSVT). It can help to terminate re-entrant tachycardias that involve the atrioventricular (AV) node. The manoeuvre is indicated in hemodynamically stable patients with narrow complex tachycardia, especially those who are young and without significant cardiac history. It is also a diagnostic tool to assess autonomic function and can be used to evaluate vagal tone and baroreceptor function. Occasionally, it is applied to differentiate between SVT and ventricular tachycardia by its effects on heart rate.
- Contraindications: It should not be performed in patients with known severe aortic stenosis, recent myocardial infarction, or significant hemodynamic instability. It is contraindicated in patients with a risk of thromboembolism, such as those with recent deep vein thrombosis (DVT), due to the risk of dislodging a clot.
- Risks: The manoeuvre is generally safe, but it carries some risks, including the possibility of transient hypotension and dizziness. In rare cases, it can cause arrhythmias such as atrial fibrillation, or, in patients with significant coronary artery disease, angina. There is also a risk of syncope, especially if the manoeuvre is not done correctly or if the patient has underlying issues with venous return.
Physiology
- The Valsalva manoeuvre exploits the body's vagal response to changes in intrathoracic pressure. It has four phases:
- Phase 1 (Initial Pressure Increase): When the patient begins to strain, the intrathoracic pressure increases, leading to a transient rise in blood pressure and reduced venous return.
- Phase 2 (Strain): Sustained straining causes reduced venous return to the heart, leading to a drop in cardiac output and a compensatory increase in heart rate.
- Phase 3 (Release of Strain): The release of pressure causes a rapid decrease in intrathoracic pressure, allowing blood to return to the heart and potentially causing a reflexive decrease in heart rate.
- Phase 4 (Reflexive Increase in Vagal Tone): As the blood returns, there is a rapid increase in cardiac output, leading to a reflex increase in vagal tone, which can slow the heart rate and potentially terminate an SVT.
- The modification of the Valsalva manoeuvre with a postural change aims to increase the effectiveness of the vagal response by enhancing venous return, thus amplifying the impact on the heart rate.
Procedure
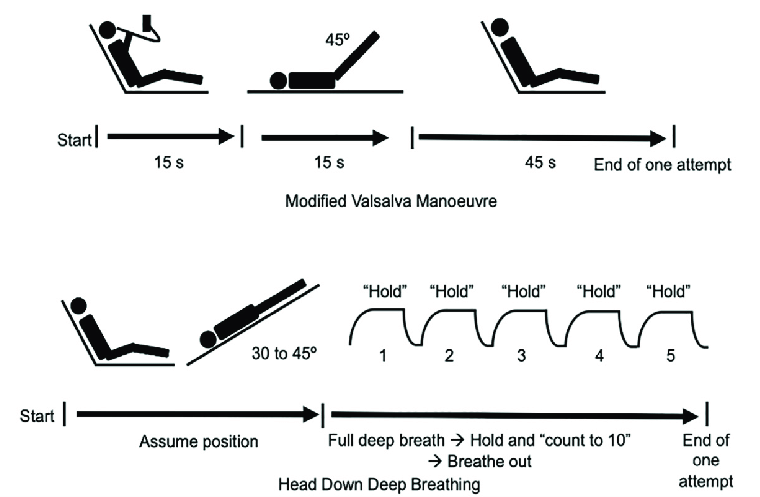
- Procedure: Strain Phase: The patient is seated or lying semi-reclined at a 45-degree angle. Instruct the patient to blow into a syringe (or similar device) with the aim of generating about 40 mmHg of pressure for 15 seconds. Blowing into the syringe creates resistance, similar to trying to inflate a blocked balloon. This increases pressure in the thorax, leading to a decrease in venous return and increased vagal tone.
- Postural Change Phase: Immediately after the strain, lay the patient flat while simultaneously lifting their legs up to a 45-degree angle for 15 seconds. This position change increases venous return to the heart and enhances the vagal response triggered by the strain phase.
- Recovery Phase: After 15 seconds, lower the patient’s legs and sit them back up. Monitor the patient's response and assess if the tachycardia has resolved. If successful, the manoeuvre should result in a slower, regular heart rhythm.
- Effectiveness: The modified Valsalva manoeuvre is more effective than the standard Valsalva manoeuvre, with success rates around 43% compared to the 17% success rate of the standard version. The postural change component helps to significantly increase venous return, thus enhancing the parasympathetic response and increasing the likelihood of terminating the tachycardia.
Post Procedure
- Follow-Up Care: If the modified Valsalva manoeuvre is successful in terminating the SVT, the patient should be observed for recurrence and assessed for potential triggers of their arrhythmia. Further investigations such as an ECG or echocardiogram may be necessary to evaluate any underlying structural heart disease. If the SVT persists despite the manoeuvre, pharmacological intervention with adenosine may be considered as the next step.
- References: For more detailed guidance on performing the modified Valsalva manoeuvre, refer to National Centre for Biotechnology Information (NCBI) and American Heart Association Journals.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery